A breathtakingly rare presentation of pyloric stenosis
Sir,
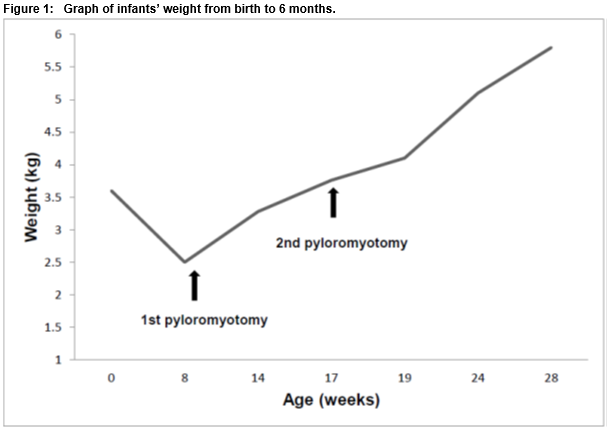
A nine-week-old male infant presented in extremis following a one week history of effortless, non-bilious vomiting. Weighing 2.5kg, he was 30% below birthweight and had Cheyne-Stokes respiration. Severe hypochloraemic, hypokalaemic metabolic alkalosis (pH 7.72, pCO2 6.5 kPa, bicarbonate 70.9 mmol/L, Base Excess 44.7, potassium 1.9mmol/L, chloride <60mmol/L) was present. Ultrasound confirmed the diagnosis of infantile hypertrophic pyloric stenosis (IHPS) (pyloric channel length 24mm, muscle thickness 7mm). Following stabilisation, he underwent a Ramstedt pyloromyotomy and his recovery was uneventful.
Two months later, after an interval weight gain of 1.2kg (Figure 1), his symptoms along with a severe metabolic alkalosis (pH 7.70) recurred and imaging again confirmed IHPS (pyloric channel length 20 mm, muscle thickness of 4.5 mm). Intraoperatively, the hypertrophic muscle was divided at a second point after observing that the initial split was intact.
Metabolic alkalosis-induced respiratory depression has been reported just twice previously in IHPS1,2. In the presence of significant metabolic derangement, these infants need to be closely monitored for apnoea and hypoventilation.
IHPS occurs almost exclusively in infants younger than three months. True recurrence is confirmed by intraoperative findings and requires an asymptomatic period with no vomiting, interval weight gain and normal feeding following initial pyloromyotomy. This is an extremely rare entity with just seven published cases in the literature3,4. It has been hypothesised that true recurrence is due to early operative intervention in a disease process which is still in evolution4. To date, all true recurrences have been in infants whose initial presentation was at a median (range) of 19 (10-27) days with representation after a period of three to four weeks. In this case, initial presentation was significantly later at nine weeks and the interval to representation a further eight weeks later indicating that the process of pyloric muscle hypertrophy can be more slowly progressive and prolonged beyond that previously reported in the literature. The slow progression of pyloric hypertrophy likely contributed to the severe metabolic alkalosis identified on both occasions.
SA Hurley1 FMcCartan1 NMcGrath2 AMortell3 MJ O’Grady1
1Department of Paediatrics, Midland Regional Hospital, Mullingar, Ireland
2Department of Paediatrics, Children’s University Hospital, Temple St., Dublin 1, Ireland
3Department of Paediatric Surgery, Children’s University Hospital, Temple St., Dublin 1, Ireland
Corresponding author
Dr Michael O’Grady
Department of Paediatrics, Midland Regional Hospital, Mullingar, Ireland
Email: [email protected]
Refrences
1. Pappano D. Alkalosis-Induced Respiratory Depression from Infantile Hypertrophic
Pyloric Stenosis. Pediatr Emerg Care 2011; 27:124
2. Tigges CR, Bigham MT. Hypertrophic Pyloric Stenosis: It Can Take Your Breath
Away. Air Med J 2012; 31:45-8
3. Al-Ansari A, Altokhais TI. Recurrent pyloric stenosis. Pediatr Int 2016; 58:619-21.
4. Parigi GB, Verga G. Late recurrence of infantile hypertrophic pyloric stenosis. Pediatr Surg Int 1994; 9:409-10.
(P555)