Introduction
Retropharyngeal abscesses (RPA) are deep neck space infections that can pose an immediate life-threatening emergency, such as airway obstruction. [1] The potential space can become infected by bacteria spreading from a contiguous area [2] or direct inoculation from penetrating trauma. [3] Infection is often polymicrobial (most commonly group A beta-hemolytic streptococci). [4]
Methods
We describe an atypical presentation of RPA in a three-year-old girl who attended with a history of post-traumatic neck pain.
Case Report
MB presented to the Emergency Department with neck pain and reduced range of motion following a kick to the neck by a sibling. Her mother reported it as a mild trauma, with disproportionate pain afterwards. Of note, MB had an ongoing URTI for which she had been treated with antibiotics one week previously. On examination, MB was irritable and held her head in slight flexion, resisting any neck movements. Her pain was severe, requiring opiate analgesia. She was hemodynamically stable and apyrexic. Her tonsils were not inflamed and she had no signs of inflammation of the posterior pharyngeal wall. Blood tests revealed a normal white cell count with a raised CRP (50) and ESR (99). Given the history of trauma, a cervical spine x-ray was performed which showed pseudo subluxation of C2/C3 with a concern regarding facet joint injury, which was further characterized by CT. As physicians were focused on the bony structures, pre-vertebral soft tissue swelling (which was visible on both x-ray and CT) was overlooked. Ultimately, MRI revealed a RPA without any traumatic bone injury (Illustrated in the image below). The RPA was incised and drained. Cultures grew H.influenzae for which she was treated with antibiotics. She recovered well without any negative sequelae.
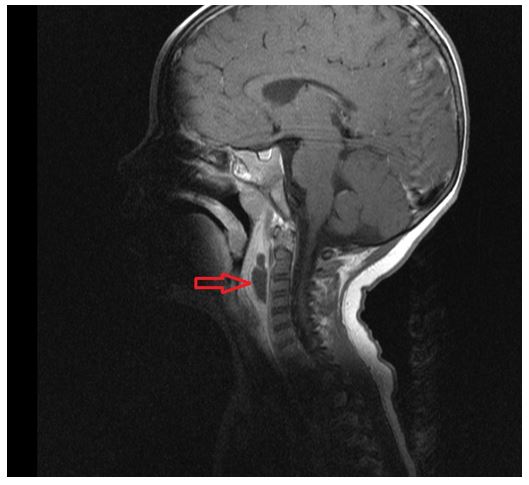
Arrow = Abscess
Discussion
In this case the presenting history of mild trauma did not explain the clinical picture of our patient, and MB did not have any classic signs and symptoms of RPA. It may also be well possible that the recent course of antibiotics, masked her symptoms.
Influenced by the history of trauma, physicians both arranged and interpreted imaging with a view to identifying bony injury. Although pseudo subluxation at C2/C3 is a recognized finding in children,[5] the history of trauma was concerning. Therefore, a non-contrast CT was performed to visualize the vertebrae and facet joints, albeit sacrificing soft tissue detail to reduce radiation dose. MRI ultimately defined the RPA however in retrospect; swelling of the prevertebral soft tissues was visible on both the x-ray and CT.
This case highlights an unusual presentation of a retropharyngeal abscess, and reminds us that trauma can often be a red herring in a patient’s presentation.
Conflicts of Interest Statement
The authors declare no conflict of interest.
Corresponding Author
Abdullah Rana,
Department of Emergency Medicine,
University Hospital Galway, Galway.
Email: [email protected]
References
1. McLeod C, Stanley KA (January 2008). "Images in emergency medicine: retropharyngeal abscess". West J Emerg Med. 9 (1): 55. PMC 2672230 . PMID 19561707.
2. Choi SS, Vezina LG, Grundfast KM (1997): Relative incidence and alternative approaches for surgical drainage of different types of deep neck abscesses in children. Arch Otolaryngol Head Neck Surg, 123:1271-1275.
3. Afolabi OA, Fadare JO, Oyewole EO, Ogah SA (2011). Fish bone foreign body presenting with acute fulminating retropharyngeal abscess in a resource challenged center: case report. J Med Case Reports. Apr 27;5(1):165.
4. RAFTOPULOS MH, JEFFERSON ND, KERTESZ T. Retropharyngeal abscess in a six-week-old child: an approach to management. JRSM Short Rep [online] 2013, 4(11):2042533313499558 [viewed 23 August 2014] Available from: doi:10.1177/2042533313499558
5. Shaw M, Burnett H, Wilson A,.Pseudosubluxation of C2 on C3 in polytraumatized children – prevalence and significance. Clin Radiol1999;54:377–80.
P900