Introduction
Solitary fibrous tumours (SFT) are unusual soft tissue neoplasms that originate mostly from the visceral pleura. Extra-pleural sites of origin include; soft-tissue, sites of head and neck origin, retro-peritoneum and rarely the urological tract. SFTs are described as “typical” or “malignant”. Approximately 10% of tumours display malignant characteristics, however, the morphological and clinical course are not strongly correlated1. Additionally, cases of extra-thoracic primary SFT are associated with late recurrence and therefore appreciation of this is required2. We present a rare case of metastatic pulmonary Solitary Fibrous Tumour presenting 11 years post resection of renal primary Solitary Fibrous Tumour.
Case
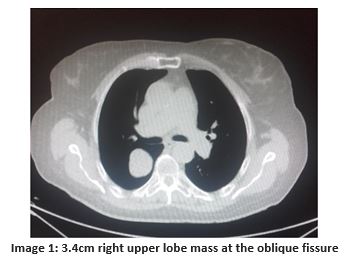
A 74 year old female smoker was found to have a right upper lobe mass with surveillance CT imaging. Her background was significant for left-sided partial nephrectomy for renal solitary fibrous tumour 11 years previously. The patient was asymptomatic. Clinical examination was normal. . CT imaging demonstrated a 3.4cm right upper lobe mass at the oblique fissure with extension into the right lower lobe (image 1). PET CT demonstrated FDG uptake (SUV 2.9) with no evidence of local recurrence, nodal involvement or other metastases.
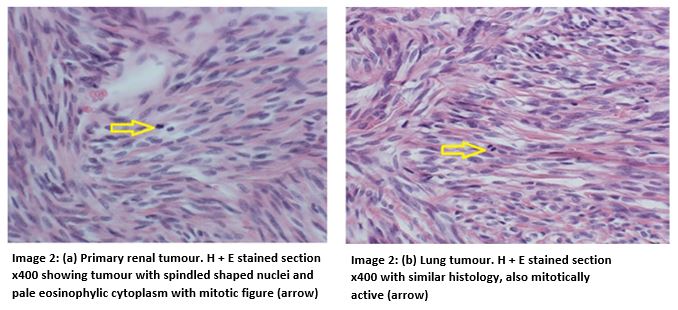
 Subsequently, the patient underwent uniportal video-assisted thorascopic surgery (VATS) for initial inspection converted to open thoracotomy excision of the tumour. Apical segmentectomy of the right lower lobe and wedge resection of the right upper lobe with lymphadenectomy was performed. The patient’s post-operative course was uneventful and she was discharged day 12 post surgery. Postoperative histology showed features consistent with SFT, similar to that seen in the previous renal tumour. The tumour had a mitotic count of 12 mitoses per 10 high power fields. It also showed the presence of moderate pleomorphism, haemorrhage and necrosis (image 2). An R0 resection was achieved. Consensus from the multidisciplinary team meeting was that no adjuvant therapy was warranted.
Subsequently, the patient underwent uniportal video-assisted thorascopic surgery (VATS) for initial inspection converted to open thoracotomy excision of the tumour. Apical segmentectomy of the right lower lobe and wedge resection of the right upper lobe with lymphadenectomy was performed. The patient’s post-operative course was uneventful and she was discharged day 12 post surgery. Postoperative histology showed features consistent with SFT, similar to that seen in the previous renal tumour. The tumour had a mitotic count of 12 mitoses per 10 high power fields. It also showed the presence of moderate pleomorphism, haemorrhage and necrosis (image 2). An R0 resection was achieved. Consensus from the multidisciplinary team meeting was that no adjuvant therapy was warranted.
Discussion
Solitary fibrous tumours are described as mesenchymal spindle cell tumours3. Previously referred to as hemangioperiocytomas, the incidence of SFT has been reported as 0.2/100,000/year(2). Renal presentation of SFT is rare and less than 50 cases have been reported in the literature to date1, 3. Metastatic pulmonary disease from a renal primary SFT is more rare. SFT are asymptomatic in approximately 50% of patients but may present with local symptoms such as pain or mass effects, systemic symptoms or paraneoplastic syndromes4.
Solitary fibrous tumours can rarely exhibit metastatic behaviour to sites such as the lung, liver or bone via haematogenous spread3. Pathological features and clinical course are poorly correlated and therefore difficulties arise in predicting metastasis2. The description of a SFT as “malignant” is based on a mitotic count >8/10 high power field count and the presence of gross haemorrhage, pleomorphism and necrosis. Tumours with benign or typical features may also follow a malignant course however. Relapse of disease may occur late, at an interval of more than ten years. In one series of 83 patients, the late recurrence rate was 10%2. All patients with late relapse had an extra-thoracic primary neoplasm and 42% had a “typical” histological subtype primary neoplasm2. Notably, the series found that 70% of patients had recurrence at the initial primary site but regardless of whether local or distant recurrence occurred, no patient was cured even with complete salvage surgery2. Fortunately, median survival from surgery was 8 years.
This case report serves to highlight an intriguing but purposeful reminder: although SFTs are rare it is critical to be aware of the clinical course associated with SFT. It is important to realise that the clinical course does not necessarily correspond to these boundaries. Late recurrence is associated with extra-thoracic primary tumours warranting long-term follow-up. Although complete cure is rare in cases of recurrence, prognosis is good with a median survival of 8 years post salvage surgery reported2.
Conflicts of Interest Statement
The authors have no conflicts of interest to declare.
Corresponding Author
Mr. Adam Daly,
Department of Cardiothoracic Surgery,
Cork University Hospital,
Co. Cork
Email: [email protected]
References
1. Sfoungaristos S, Papatheodorou M, Kavouras A, Perimenis P. Solitary fibrous tumor of the kidney with massive retroperitoneal recurrence. A case presentation. Prague Med Rep [Internet]. 2012 Jan [cited 2015 Aug 12];113(3):246–50. Available from: http://www.ncbi.nlm.nih.gov/pubmed/22980566
2. Baldi GG, Stacchiotti S, Mauro V, Dei Tos AP, Gronchi A, Pastorino U, Duranti L4, Provenzano S1, Marrari A1, Libertini M1, Pilotti S2, Casali PG1. Solitary fibrous tumor of all sites: outcome of late recurrences in 14 patients. Clin Sarcoma Res [Internet]. BioMed Central Ltd; 2013 Jan 3 [cited 2015 Aug 12];3(1):4. Available from: http://www.clinicalsarcomaresearch.com/content/3/1/4
3. Mearini E, Cochetti G, Barillaro F, Fatigoni S, Roila F. Renal malignant solitary fibrous tumor with single lymph node involvement: report of unusual metastasis and review of the literature. Onco Targets Ther [Internet]. 2014 Jan [cited 2015 Aug 12];7:679–85. Available from: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=4020903&tool=pmcentrez&rendertype=abstract
4. Zhu Y, Du K, Ye X, Song D, Long D. Solitary fibrous tumors of pleura and lung: report of twelve cases. J Thorac Dis [Internet]. 2013 Jun [cited 2015 Aug 12];5(3):310–3. Available from: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=3698259&tool=pmcentrez&rendertype=abstract
Issue: Ir Med J; Vol 112; No. 6; P954