Introduction
Epidemiological and genetic observational studies have shown evidence of an association between vitamin D deficiency and risk of development of MS1. An inverse relationship between vitamin D levels and MS activity on MRI has also been identified2. While vitamin D supplementation in MS has shown beneficial immunomodulatory effects3 there is no evidence in the randomised controlled trials conducted to date of a clinical effect4,5. The optimal approach for supplementing vitamin D in MS, or the optimal serum levels to target, have not been defined. As vitamin D is easily available over-the-counter and online, it may be difficult to regulate individual patients who are self-supplementing.
Case report
A 45 year-old male presented to the E.D. with eight days of nausea, vomiting, lethargy, anorexia and constipation. He was wheelchair-bound with a diagnosis of MS. He reported that he had not attended neurology follow-up for the past seven years. Initial bloods on admission showed severe hypercalcaemia (corrected calcium of 3.69mmol/L), and an acute kidney injury (see table 1).
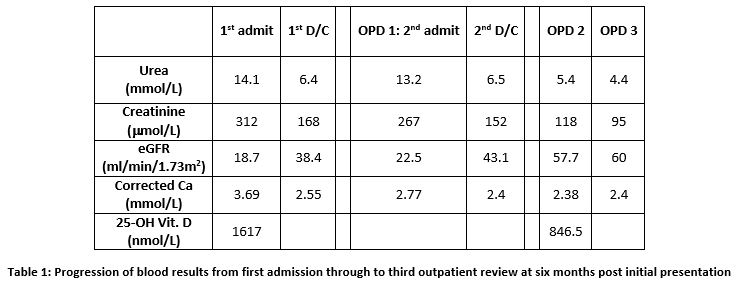
Initial management involved intravenous 0.9% NaCl rehydration, anti-emetics, and laxatives for constipation. Further questioning found that the patient had been taking 6 internet-bought supplements, one of which was vitamin D3. He reported an intake of 10,000IU daily for close to two years. His 25-OH-vitamin D level after serial dilution was 1617nmol/L.
Along with IV rehydration, he initially received prednisolone and calcitonin to treat his severe hypercalcaemia. Once rehydrated and some recovery of renal function was achieved, he received IV zolendronic acid. He was discharged home for follow-up in OPD 2 weeks later when he required re-admission for further rehydration but no further additional treatment. At subsequent outpatient follow-up calcium has remained normal and renal function has normalised.
Discussion
There is increasing evidence to support a beneficial effect of vitamin D on the inflammatory component of MS, and correction of vitamin D insufficiency in MS patients is recommended1. Routine supplementation in sufficient patients may be seen more frequently in clinical practice and a multicenter, randomised, double-blind controlled trial of vitamin D in multiple sclerosis is currently ongoing6. A 2016 study assessed safety and immunologic effects of high versus low vitamin D in relapsing-remitting MS patients with a baseline 25-OH Vitamin D level >50nmol/L. It concluded that a high dose of 10,400IU/day of vitamin D3 for a six-month period was safe and tolerable with none of the 19 patients developing hypercalcaemia3. Our patient had a similar daily intake but over a longer period of time. Importantly, his immobility may have also made him more susceptible to hypercalcaemia.
The widespread availability of vitamin D3 over-the-counter and on the internet allows patients, such as ours, to self-supplement, without monitoring of their vitamin D or calcium levels. The actual vitamin D3 content of the supplements taken may also not be regulated. This was highlighted in a case report in 2001 which described a 42 year-old man who presented with hypercalcaemia due to vitamin D intoxication after two years of self-supplementation with an over-the-counter preparation7. Analysis of different samples of the supplement revealed an actual vitamin D3 content 26 to 430 times that listed by the manufacturer. Our patient’s supplement content was not analysed but it would be feasible that the vitamin D3 content was greater than that listed.
This case highlights the importance of monitoring patients prescribed vitamin D supplementation in high doses, particularly as widespread prescribing in MS may become more common. When indicated, licensed vitamin D products should be prescribed and patients advised not to self-supplement. This case also reinforces the importance of a thorough medication history including supplements patients may be taking without knowledge of their primary or specialist treating physician.
Conflicts of Interest Statement
The authors have no conflicts of interest to declare.
Corresponding Author
Dr. Edmund Duffy,
University Hospital Limerick,
Limerick,
Ireland.
Email: [email protected]
References
1. Pierrot-Deseilligny C, Souberielle JC. Vitamin D and multiple sclerosis: An update. Mult Scler Relat Disord. 2017;14:35-45.
2. Mowry EM, Waubant E, McCulloch CE, Okuda DT, Evangelista AA, LIncolm RR, Gourraud PA, Brenneman D, Owen MC, Qualley P, Bucci M, Hauser SL, Pelletier D. Vitamin D status predicts new brain magnetic resonance imaging activity in multiple sclerosis. Ann Neurol. 2012;72(2):234-40.
3. Sotirchos ES, Bhargava P, Eckstein C, Van Haren K, Baynes M, Ntranos A, Gocke A, Steinman L, Mowry EM, Calabresi PA. Safety and immunologic effects of high- vs low-dose cholecalciferol in multiple sclerosis. Neurology. 2016;86(4):382-90.
4. Stein MS, Liu Y, Gray OM, Baker JE, Kolbe SC, Ditchfield MR, Egan GF, Mitchell PJ, Harrison LC, Butzkueven H, Kilpatrick TJ. A randomized trial of high-dose vitamin D2 in relapsing-remitting multiple sclerosis. Neurology. 2011;77(17):1611-8.
5. Kampman MT, Steffensen LH, Mellgren SI, Jorgensen L. Effect of vitamin D3 supplementation on relapses, disease progression, and measures of function in persons with multiple sclerosis: exploratory outcomes from a double-blind randomised controlled trial. Mult Scler. 2012;18(8):1144-51.
6. Bhargave P, Cassard S, Steele SU, Azevedo C, Pelletier D, Sugar EA, Waubant E, Mowry EM. The vitamin D to ameliorate multiple sclerosis (VIDAMS) trial: study design for a multicenter, randomized, double-blind controlled trial of vitamin D in multiple sclerosis. Contemp Clin Trials. 2014;39(2):288-93.
7. Koutkia P, Chen TC, Holick MF. Vitamin D Intoxication Associated with an Over-the-Counter Supplement. N Engl J Med. 2001;345(1):66-67.
Issue: Ir Med J; Vol 112; No. 6; P953