Introduction
Hurling (males) and camogie (females) are two of Ireland’s national games and are one of the fastest field sports in the world1. Hurling and camogie are predominately played in Ireland but are also played in the UK, USA, Canada and Australia2. They are amateur sports, governed by the Gaelic Athletic Association (also known as the GAA)3 and the Camogie Association. To play the game an ash stick, termed a hurley, is used to propel a hard leather ball called a sliotar2. The sliotar is made of cork which is covered with a leather wound string and weighs 100g-130g with a circumference of 23cm-25cm4. Each team consists of fourteen outfield players and one goalkeeper, who play on a rectangular pitch 145m in length and 90m wide5. The aim of the game is to score by hitting the sliotar between the oppositions goalpost and passed the goalkeeper, or over the bar2. The sliotar can be propelled through the air at velocities as high as 160km/hr or likewise along the ground2.
In order to reduce the risk of head, face and ocular injuries, the GAA introduced mandatory wearing of helmets fitted with a faceguard in three stages. Firstly, in 2005, those aged less than 18 were required to wear them, in 2007 it was expanded to include players playing under 21 and ultimately mandatory for all ages, levels or gender in 20101. Wearing a helmet fitted with a faceguard reportedly reduces the risk of hurling-related head injuries among players that presented to A&E 10-fold1. In addition, Khan et al.4 found that in the south-east of Ireland, ocular injuries significantly decreased in those aged under 18 after the introduction of the mandatory helmet rule in minor players. Despite these apparent reductions, it is anecdotally reported that players modify their faceguards, potentially to improve their central or peripheral vision and to improve their ability to track the flight of the sliotar6. This is despite the fact that modification of the helmet or faceguard is against GAA regulations as it can potentially increase serious injury risk. In fact, a case series published in 2015, highlighted that despite the compulsory use of helmets with faceguards, serious eye injuries still occur6. To the author’s knowledge, since the introduction of mandatory helmet wearing, no research has examined how common modifications to helmets and faceguards are in hurling or camogie. In addition, as of yet, the rationale behind helmet choice has yet been examined. Therefore, the aim of this study is to identify how common modifications are in hurling and camogie, why players modify their helmet and faceguards and what changes do they commonly make.
Methods
An online self-report questionnaire consisting of 27 multiple-choice questions was developed examining: helmet choice, when they wear their helmets, injuries sustained when not wearing a helmet, modifications of helmets and faceguards, their beliefs around why they modify their helmets/faceguards, and their view on future education around helmet/faceguard safety. A pilot study was completed and it was found that players took an average of 4.04±0.99 minutes to complete the questionnaire. Ethical approval was obtained from the local research ethics committee. Participants were required to read a plain language statement and provide informed consent prior to completing the questionnaire. Social media, emails to both club and county secretaries, as well as word of mouth were used to recruit players. Three hundred and four hurling and camogie players aged over 18 (188 [62%] hurlers, 116 [38%] camogie players) completed the questionnaire.
Results
Primarily hurlers filled in the questionnaire (188, 62%), compared to camogie players (116, 38%). Players reported the appearance of the helmet was the primary reason for their helmet choice (42.7%), price was also an important factor (20.3%), with just 1.6% citing safety. The majority of players wear their helmets during team training (82%), however during individual training, just 24% wear a helmet. Seventy-five percent of players reported that they were not fitted correctly when purchasing their helmet.
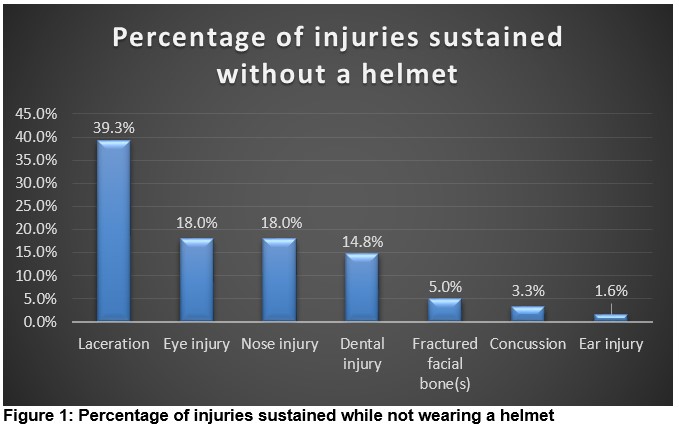
Thirty-one percent of players admitted to modifying their own helmet/faceguard and 8.0% actually reported that their helmet/faceguard was already modified when they purchased it. Guard replacement (80.0%) was the most common modification, followed by removal of bars (13.3%). In addition, 47.9% of participants knew more than 7 other players who modified their helmet. Those that knew of another player that modified their helmet/faceguard, reported that they believed they had primarily changed their faceguard, followed by removal of bars and bending of the bars on the faceguard. Players reported that they modified their helmet, primarily due to vision restriction, comfort and their perceived view that the helmet/faceguard was of poor quality. When asked if they sustained any head, face, eye or ear injuries while not wearing a helmet when playing hurling/camogie (during team or individual training), those that stated yes, sustained primarily lacerations, eye and nose injuries (Figure 1).
The majority (75.8%) of players believed that it would be beneficial if players were educated further on helmet safety and the possible increased risks associated with helmet modifications. Players believed that educational videos (40.0%) would be the most beneficial method of education, followed by a practical demonstration (27.3%), a power point presentation (19.0%) and leaflets/hand-outs (13.7%).
Discussion
Just under a third of players admitted to modifying their own helmet/faceguard, with 8% reporting that it was already modified when they purchased it. In addition, just under a half of players knew more than 7 other players that have previously modified their helmet/faceguard. This is the first study to examine the prevalence of modifications in hurling and camogie since helmets have become mandatory, and highlights that it is a potential issue due to the consequential increased risk for serious injury to the eye, face, and ear. When modifications did take place, they were primarily to the faceguard. In fact, 9.5% of hurling related eye injuries in minors that presented to an A&E from 2003-2006 were wearing a modified faceguard at the time of injury4. The findings of the current study support previous theories, that players modify their faceguards to improve their vision6. However, players also mentioned that they implemented modifications to improve the comfort of the helmet and because they perceived the helmet/faceguard was of poor quality. Further research into these aspects is needed in order to improve helmet comfort and quality to ensure players do not have a need to complete any modifications themselves. Potentially player position may influence whether a player modifies their helmet, with improvements to their visual field a primary concern of goalkeepers. Future research should examine whether modifications are more prominent in certain playing positions to facilitate targeted interventions. Kent, in 20156 suggested key recommendations to the GAA that still are applicable currently and have yet to be implemented. Helmets should be worn at all times during any trainings, matches or individual activity where the hurley and sliotar is in use. In addition, a rule change, such as mandatory checks on helmets and faceguards by referees prior to matches, to ensure no modifications have been completed should be introduced, similar to the boots check completed in soccer. During this transition period following the mandatory introduction of helmets that required players that did not frequently wear helmets to begin wearing them, modifications may be more commonplace. However, as underage players now wear helmets from the beginning of their playing career, helmet usage may potentially improve and modifications reduce.
Safety is not an important factor in the decision making process for players when choosing a helmet, with appearance and price more primary concerns. In addition, despite the fact that helmet use is mandatory for the game of hurling and camogie, some players did report that they do not wear a helmet during team training (18%), with 76% of players not wearing a helmet during individual training. Those that did experience an injury to their head, face and ear while not wearing a helmet during hurling and camogie, primarily sustained lacerations, eye and nose injuries. However, a limitation of this questionnaire is that it was unable to identify how common these injuries were with respect to exposure to hurling and camogie. In addition, this information was captured retrospectively using a questionnaire format, which is not ideal, and future research should implement a prospective examination on injuries due to modifications. Thus, it is critical that players are educated on the importance of wearing a helmet with an appropriate faceguard at all times, not solely during matches, but also throughout the full training session (including the warm-up) and individual training activities where the sliotar is in use. In fact, Kent et al.6 highlighted the warm up in particular as a potential at risk situation where players may not see the importance of helmet use and display a somewhat casual view on the potential injury risk.
Education on this importance and the specific injury risks that can occur while not wearing a helmet is critical and it is welcoming to see that the majority of players believed it would be helpful to introduce education on helmet and faceguard safety, including specifically addressing helmet and faceguard modifications. Forty percent of players would prefer educational videos as the method of addressing this issue, which has the potential to be easily implemented and disseminated to members by the GAA and the Camogie Association on their website, social media and through the media.
Future research should examine the influence modifications of helmets and faceguards has on injury risk in hurling and camogie. Educating hurlers and camogie players on the importance of helmet usage during all hurling or camogie related activities, and the inherent increased risk associated with helmet or faceguard modification should be prioritised to improve the welfare of players.
Corresponding author:
Dr Siobhán O’Connor, H270A, School of Health and Human Performance, Dublin City University, Dublin 9, Ireland.
Email: [email protected]
Conflict of Interest
The authors declare no conflict of interest. No funding has been received for the above work.
References
1. Crowley P, Crowley M. Dramatic impact of using protective equipment on the level of hurling- related head injuries: an ultimately successful 27 year programme. British Journal of Sports Medicine. 2014;48(2):147-150.
2. Blake C, O’Malley E, Gissane C, Murphy J. Epidemiology of injuries in hurling: a prospective study 2007-2011. BMJ Open. 2014;4(6):1-7.
3. Flynn T, Fennessey K, Horgan N, Walsh B, O’Connell E, Cleary P, Bealty S. Ocular injury in hurling. British Journal of Sports Medicine. 2005;39(6):493- 6.
4. Khan M, Flynn T, O’Connell E, Stack J, Beatty S. The impact of new regulations on the incidence and severity of ocular injury sustained in hurling. Eye. 2008;22(4):475- 8.
5. O’ Connor S, McCaffrey N, Whyte E, Moran K. Epidemiology of injury in male adolescent Gaelic Games. Journal of Science and Medicine in Sport. 2015;19(5):384- 8.
6. Kent, D. Eye safety in hurling: a few remaining blind sports? Irish Journal of Medical Science. 2015;184(3):707-11.
(P727)