Introduction
Pneumocephalus is defined as the presence of intracranial air. This is most commonly secondary to traumatic head injury1. Computed Tomography (CT) is the gold standard for diagnosing pneumocephalus2. The majority of cases are managed conservatively unless there is evidence of raised intracranial pressure in which case urgent decompression is warranted to prevent a catastrophic outcome3.
Case
A 52-year-old gentleman presented to the emergency department following an assault earlier that day. He was alert and ambulatory with a Glasgow Coma Scale of 15. He had no recollection of the event and only reported a mild frontal headache. Initial physical inspection was remarkable for signs of a base of skull or mid-face fracture. There were no other signs of injury. No abnormality was found on neurological exam. Initial investigation with plain radiograph of the facial bones revealed extensive pneumocephalus (Figure 1). Bilateral frontal bone, orbital and maxillary fractures were also noted.
Figure 1.

He proceeded to have a CT scan of the head and facial bones which confirmed complex facial bone fractures with extensive pneumocephalus. The Mount Fuji sign was present indicating tension pneumocephalus (Figure 2). This sign refers to the presence of air between the frontal lobes separated by the adhering cortical veins, giving the appearance of the iconic mountain peak in Japan1,2.
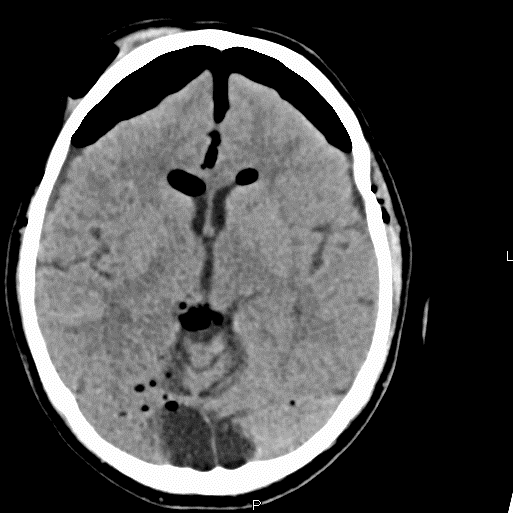
Figure 2.
Urgent neurosurgical opinion was sought in this patient’s case, and conservative management was recommended. He remained stable throughout his 16 day hospitalization and did not require any further neuroimaging. At the time of discharge, he was well with no neurological impairment.
Discussion
Pneumocephalus is defined as the presence of intracranial air. It is an uncommon complication of traumatic head injury, affecting 0.5-1% of cases3. Air is most likely to enter the cranium through a fracture of the para-nasal sinuses as in this case. Fractures of the middle ear cavity or less likely depressed skull fractures are other recognised traumatic aetiologies2,4. Pneumocephalus is also associated with neurosurgery, barotrauma, nasopharyngeal tumour invasion and meningitis5. In the majority of cases pneumocephalus is asymptomatic6. If there is a valve mechanism present, trapped expansion of intracranial air can result in headache and signs and symptoms of increased intracranial pressure. In such cases it is referred to as a tension pneumocephalus and may require urgent craniotomy to prevent a catastrophic outcome7. CT is the gold standard for diagnosing pneumocephalus. Radiological tension pneumocephalus usually necessitates urgent craniotomy but in this case the patient showed no clinical evidence of raised intracranial pressure and was able to be managed conservatively1,9.
Most cases of pneumocephalus will resolve with conservative management. This involves maintaining a supine position initially, normobaric oxygenation, avoidance of the Valsalva manoeuvre (such as coughing or sneezing), and administration of antibiotics especially in depressed skull fractures secondary to trauma10. When symptoms and signs of raised intracranial pressure appear treatment is focussed upon urgent decompression which can include burr holes, needle aspiration and closure of the dural tear7. This is a rare case of radiological tension pneumocephalus which did not require operative management.
Correspondence:
James Ryan
Emergency Department, Mater Misericordiae University Hospital, Eccles St, Dublin.
Email: [email protected]
Conflicts of interest:
On behalf of all authors, the corresponding author states that there are no conflicts of interest.
References:
1. Leong KM, Vijayananthan A, Sia SF, Waran V. Pneumocephalus: an uncommon finding in trauma. Med J Malaysia. 2008 Aug;63(3):256–8.
2. Osborn AG, Daines JH, Wing SD, Anderson RE. Intracranial air on computerized tomography. J Neurosurg. 1978 Mar;48(3):355–9.
3. Dabdoub CB, Salas G, Silveira E do N, Dabdoub CF. Review of the management of pneumocephalus. Surg Neurol Int. 2015;6:155.
4. Michel SJ. The Mount Fuji sign. Radiology. 2004 Aug;232(2):449–50.
5. Mattick A, Goodwin P. Mount Fuji sign on CT following trauma. J Trauma. 2005 Jul;59(1):254.
6. Rathore AS, Satyarthee GD, Mahapatra AK. Post-Traumatic Tension Pneumocephalus: Series of Four Patients and Review of the Literature. Turk Neurosurg. 2016;26(2):302–5.
7. Markham JW. The clinical features of pneumocephalus based upon a survey of 284 cases with report of 11 additional cases. Acta Neurochir (Wien). 1967;16(1):1–78.
8. Krishnan K, Paterson S, Adhiyaman V. Pneumocephalus. QJM. 2011 Dec;104(12):1097.
9. Agrawal A, Singh BR. Mount Fuji sign with concavo-convex appearance of epidural haematoma in a patient with tension pneumocephalus. J Radiol Case Rep [Internet]. 2009 Jan 1;3(1):10–2. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3303266/
10. Karavelioglu E, Eser O, Haktanir A. Pneumocephalus and pneumorrhachis after spinal surgery: case report and review of the literature. Neurol Med Chir (Tokyo). 2014;54(5):405–7.
(P550)