Introduction
SS is a rare neurodegenerative disorder caused by chronic subarachnoid haemorrhage. Clinically, the cardinal features are progressive sensorineural deafness and cerebellar ataxia. Brain magnetic resonance imaging has made antemortem diagnosis of this condition feasible. Imaging of the entire neuraxis should be done to identify any treatable cause.
Case Report
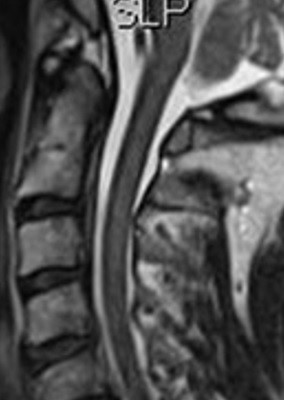
A 69 year old male presented with a five year history of unsteadiness, progressive hearing impairment and bilateral lower limbs tingling. Neurological examination revealed bilateral sensory deafness and gait ataxia. Pure-tone audiometry results were consistent with bilateral sensorineural deafness. Magnetic resonance imaging of the brain and spine showed hypointensity surrounding the brainstem, superior cerebellar fissures (Figure 1) and extending into the proximal cervical cord (Figure 2) in keeping with superficial hemosiderin deposition. Magnetic resonance angiography of the brain was normal.
Figure 1: Zoomed axial view MRI of the brain showing hypointensity surrounding the brain stem and superficial cerebellar fissures.
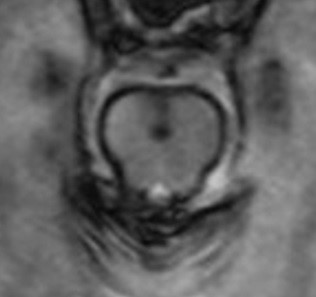
Figure 2: Zoomed sagittal view MRI of cervical spine demonstrates hypointensity
Discussion
SS is a neurodegenerative disorder caused by chronic haemorrhage within the subarachnoid space leading to deposition of hemosiderin in subpial layers of the brainstem, cerebellum and spinal cord. The cardinal features of SS of the CNS are deafness and cerebellar ataxia, and these occur in approximately 90% of cases1. Less common manifestations include myelopathy, bladder disturbance, anosmia and dementia. Although uncommon, other cranial nerves involvement have also been reported in SS, including optic nerve, trigeminal nerve and extraocular nerve palsies. Predisposing factors include prior history of head trauma, intradural surgery, cerebral amyloid angiopathy, CNS tumours, brachial plexus injury and other causes of subarachnoid haemorrhage. The aetiology is not identified in up to 35% of cases2. The condition has a predilection for the cerebellum and the eight cranial nerve. This may be explained to some extent by blood pooling in the posterior fossa. In addition, the eight nerve has a long glial segment that predisposes it to iron deposition and hence axonal injury3. Finally, the presence of Bergmann glial cells in the cerebellum that display increased ferritin synthesis makes it preferentially affected4.
Imaging of the entire neuraxis should be done to out rule an underlying dural defects, neoplasia or arteriovenous malformations which may be amenable to surgery5. Removing the source of the bleeding may halt further disease progression but doesn’t reverse the clinical manifestations of the disorder. Few reports have shown resolution of the subarachnoid bleeding by analysing the cerebrospinal fluid post-operatively. However, it was difficult to assess the clinical outcomes in view of the slow progression of the disease. There is no effective treatment to date and previous attempts of iron chelation were unsuccessful.
Correspondence:
TM Abkur
Department of Neurology, University Hospital Galway, Galway
Email:[email protected]
References
1. Fearnley JM, Stevens JM, Rudge P. Superficial siderosis of the central nervous system. Brain 1995; 118:1051–66.
2. Scheid R, Frisch S. Schroeter ML. Superficial siderosis of the central nervous system - treatment with steroids? J Clin Pharm Ther. 2009;34:603–5.
3. Kumar N, Cohen-Gadol AA, Wright RA, et al. Superficial siderosis. Neurology 2006;66:1144–52.
4. Kumar N. Neuroimaging in superficial siderosis: an in-depth look. AJNR Am J Neuroradiol 2010;31:5–14.
5. Haroun RI, Li KW, Rigamonti D. Surgical resection of a cerebral arteriovenous malformation for treatment of superficial siderosis: case report. Surg Neurol 2000; 53:554–8
p376