Introduction
Vaginal bleeding is a common event at all stages of pregnancy, especially in the first trimester, occurring in 20 to 40 percent of pregnancies1. Early pregnancy complications make up an estimated 1% of all presentations to emergency departments2. The aetiology of these bleeds is often difficult to determine. The goal of early pregnancy assessment is to make a diagnosis when possible, and to out rule any major pathology such as ectopic or molar pregnancies. Miscarriage is a common event in early pregnancy, affecting up to 25% of pregnancies1. Prompt and accurate diagnosis and management is important, both to reduce maternal morbidity and to avoid excessive emotional distress. Training in ultrasound has traditionally followed an apprenticeship model, which has been shown to be unpredictable for improving candidate’s practical skills3. Guidelines, simulators, and hands-on skills sessions have contributed to reductions in maternal morbidity and mortality, most notably with post-partum haemorrhage3, both in the urban and rural settings4. National clinical practice guidelines recommend formal training in ultrasound imaging5. Our study aimed to evaluate the effect on trainee knowledge of a multifaceted educational programme in early pregnancy complications.
Methods
The National Maternity Hospital is a large tertiary level university maternity unit. An out-of-ours service (OHS) is provided for women at any stage in pregnancy who present with an emergency. The OHS is staffed by a clinical midwife specialist (CMS), and basic specialist trainees (BST year 1-2, trained in ultrasound), and is supported by registrar and consultant staff. All BST trainees in Obstetrics & Gynaecology were invited to participate in the study, which was deemed exempt by the hospital ethics committee. The educational programme consisted of didactic lectures reviewing national early pregnancy guidelines5,6, and simulation and practical sessions. A questionnaire reviewing early pregnancy complications (Table 1) was administered prior to and following completion of the programme. Contingency tables were analysed using Fisher’s exact test.
Results
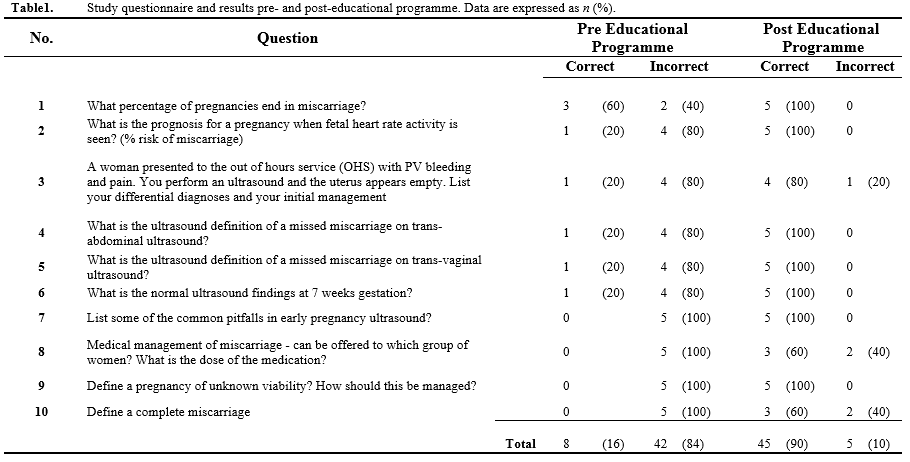
All but one participant (6/7) completed the educational programme. Five NCHDs (5/7) completed the questionnaire. The pre-education questionnaire showed a generally poor knowledge with 16% (8/50) of questions answered correctly. Following the educational programme, there was a statistically significant improvement (p<0.001) in participant knowledge, with 90% (45/50) of questions answered correctly.Trainees had a reasonable understanding of the epidemiology of miscarriage (Question 1; 3/5 correct). The largest improvement was in questions regarding definitions of early pregnancy miscarriage (2/15 vs. 13/15, p<0.0001). Following completion of the programme, participants correctly identified the percentage of pregnancies ending in miscarriage, the prognosis for a pregnancy where the fetal heart beat was identified, management of early pregnancy bleeding, ultrasound definitions of different types of miscarriage, as well as normal findings (Table 1).
Discussion
This study has demonstrated significant improvement in participant knowledge following a multifaceted educational programme in early pregnancy complications. There was improvement across all questions after the educational programme. Educational programmes are associated with an increase in knowledge retention for up to one year afterwards7. Our results are consistent with previous research, which showed that didactic lectures, combined with simulation training improved clinical knowledge8. Interestingly, this same study did not find any concomitant increase in practical skill, in contrast to other studies that have demonstrated the benefit of simulation in ultrasound training9,10. Self-guided training is a popular choice in many institutions as this reduces cost and faculty commitment, however skill acquisition has been shown to be superior with faculty led programmes, and are preferred by participants10. The small sample size and single-centre nature of our study limits the generalisability of our results, though ensures homogeneity in the delivery of the educational programme. Further work is needed to investigate the benefit to clinical practice, though we have shown the potential value of our educational programme, given its low cost, both financially and in human resources.
Correspondence: Mary Higgins
UCD Obstetrics Gynaecology, National Maternity Hospital, Holles St, Dublin 2
Email: [email protected]
References
1. Nanda K, Lopez LM, Grimes DA, Peloggia A, Nanda G. Expectant care versus surgical treatment for miscarriage. Cochrane Database Syst Rev 2012, 3:CD003518.
2. O’Rourke D, Wood S. The early pregnancy assessment project: the effect of cooperative care in the emergency department for management of early pregnancy complications. O’Rourke D1, Wood S. Aust N Z J Obstet Gynaecol 2009; 49: 110-114.
3. Rizvi F, Mackey R, Barrett T, McKenna P, Geary M. Successful reduction of massive postpartum haemorrhage by use of guidelines and staff education. BJOG 111: 495-498.
4. Perosky J, Richter R, Rybak O, Gans-Larty F, Mensah MA, Danquah A, Debpuur D, Kolbilla D, Ofosu A, Anderson F, Marzano D, Andreatta P. A low-cost simulator for learning to manage postpartum hemorrhage in rural Africa. Simul Healthc 2011 Feb;6:42-7.
5. Institute of Obstetricians and Gynaecologists (2010) Ultrasound Diagnosis Of Early Pregnancy Miscarriage. Royal College of Physicians of Ireland. http://www.rcpi.ie/content/docs/000001/647_5_media.pdf. Accessed 20 July 2015.
6. Institute of Obstetricians and Gynaecologists (2012) Management Of Early Pregnancy Miscarriage. Royal College of Physicians of Ireland. http://www.rcpi.ie/content/docs/000001/655_5_media.pdf. Accessed 20 July 2015.
7. Crofts JF, Fox R, Draycott TJ, Winter C, Hunt LP, Akande VA. Retention of factual knowledge after practical training for intrapartum emergencies. Int J Gynaecol Obstet. 2013 Oct;123:81-5.
8. Woodworth GE, Chen EM, Horn JL, Aziz MF. Efficacy of computer-based video and simulation in ultrasound-guided regional anesthesia training. J Clin Anesth. 2014 May;26:212-21.
9. Keddis MT, Cullen MW, Reed DA, Halvorsen AJ, McDonald FS, Takahashi PY, Bhagra A. Effectiveness of an ultrasound training module for internal medicine residents. BMC Med Educ. 2011 Sep 28;11:75.
10. Alba GA, Kelmenson DA, Noble VE, Murray AF, Currier PF. Faculty staff-guided versus self-guided ultrasound training for internal medicine residents. Med Educ. 2013 Nov;47:1099-108.
P394