Introduction
Ambulatory Gynaecology care involves assessment, treatment and discharge of the gynaecology patient on the same day in an outpatient setting1. This allows a ‘one stop’ approach in the management of gynaecological conditions and serves as an alternative to conventional outpatient clinics followed by inpatient surgery2. The proportion of procedures performed in an ambulatory setting in Europe, the U.S.A. and Asia is gradually increasing3. In Mayo University Hospital, Ireland, ambulatory procedures have reduced inpatient bed usage allowing ring-fencing of a reduced compliment of combined surgical-gynaecological beds without compromise of productivity4.
Abnormal uterine bleeding is common and has a notable effect on women, both clinically and socially5. In a UK study, 12% of referrals to the gynaecology outpatient clinics were due to heavy menstrual bleeding6. Women generally attend conventional gynaecology clinics on multiple occasions before evaluation is complete7. Adopting a more modern ambulatory approach in the investigation and treatment of gynaecology patients, however, needs to ensure the provision of a high-quality service which is acceptable to patients in terms of administrative elements, physical surroundings, quality of communication by caregivers, convenience and comfort experienced by the patient. This study was designed to examine these factors as part of an overall assessment of the quality of the patient’s experience during a journey through the Ambulatory Gynaecology Clinic in Mayo University Hospital.
The Ambulatory Gynaecology Clinic at Mayo University Hospital, initially established as a small office hysteroscopy clinic in the Day Services Unit in 2002, subsequently expanded in 2005 and was converted to a fully functioning Ambulatory Gynaecology Unit led by three consultants in 2008. The unit presently has a turnover of 8 – 10 patients per day. The main focus of this clinic is the management of abnormal uterine bleeding. Same-day investigations are provided including haematology, pelvic ultrasound, saline-infusion sonography, diagnostic hysteroscopy and endometrial biopsy as well as minor procedures such as cervical polypectomy, endometrial polypectomy and intra-uterine device insertion, removal or replacement. There are two treatment rooms each with a multipurpose set-up. Each room is adapted to ensure patient comfort and privacy with an adjoining toilet/changing area. A nursing staff member functions as the patient’s advocate and chaperone and provides the very important “vocal local” element of ambulatory care. The rooms are appropriately stocked with instruments essential for a one-stop menstrual clinic as well as resuscitation facilities, in accordance with recommendations from the joint British Society for Gynaecological Endoscopy / Royal College of Obstetricians and Gynaecologists Guideline on Best Practice in Outpatient Hysteroscopy8.
Methods
A questionnaire was designed to assess quality of care and patient acceptability and satisfaction with respect to the patient’s experience in the Ambulatory Gynaecology Clinic (Table 1). This questionnaire assessed the patient’s experience with respect to their referral, the clinic environment, communication within the clinic, the procedure performed, events following the procedure, overall assessment of the clinic and suggestions for improvement within the service. Three main question styles were used for the questionnaire design. A five point Likert scale of answer options was used for majority of the questions, with other questions requiring a “yes / no” answer and others requiring comments by the patients. Women attending the clinic, between the ages of 18 and 65 years, were invited to participate.
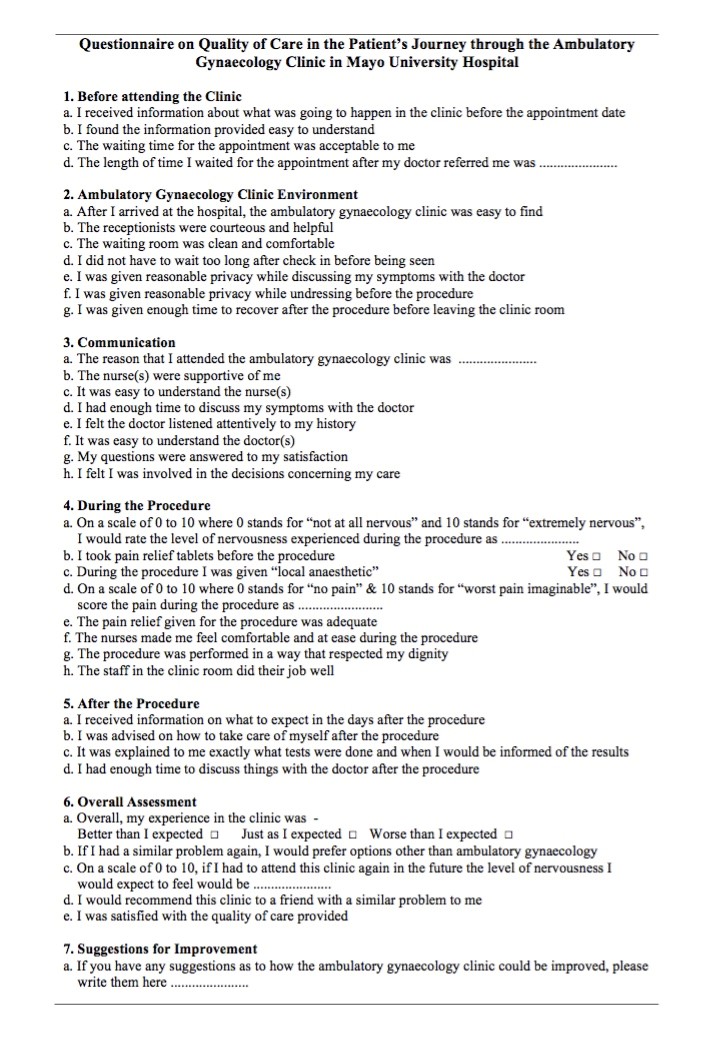 Table 1: Ambulatory Gynaecology Clinic Questionnaire - Women were asked to mark responses as strongly agree, agree, neutral, disagree, or strongly disagree
Table 1: Ambulatory Gynaecology Clinic Questionnaire - Women were asked to mark responses as strongly agree, agree, neutral, disagree, or strongly disagree
Results
Eighty-seven patients were recruited voluntarily, at the time of clinic registration, over a five-month period during 2013. Questionnaires were self-completed after the clinic visit. Seven questionnaires were excluded due to incorrect completion. Three quarters of attendees had a menstrual disorder, while 25% had other gynaecological disorders. Various gynaecological procedures were carried out, ranging from cervical polypectomy to outpatient hysteroscopy.
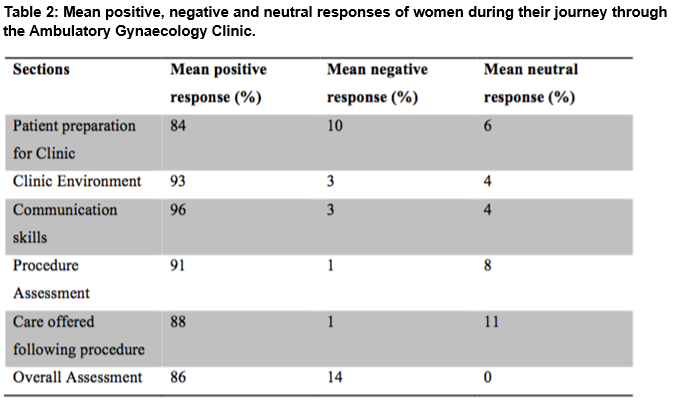
Patient preparation for clinic: Three quarters of patients acknowledged receiving prior information about their procedure before their appointment. The mean waiting time for patients’ appointments was 8 weeks. Fifty-nine per cent of patients found the information provided regarding their procedures easy to understand.
Clinic Environment: Eighty per cent of patients said the clinic was easy to find, all said the receptionist was courteous and helpful and the room was clean and comfortable, 83% said they did not have to wait long after arrival to be seen, 97% said they were given reasonable privacy while preparing immediately before the procedure and 96% of patients said they were given enough time to recover after the procedure.
Communication: There was a high level of satisfaction with regard to supportive nursing staff (97%), ease of understanding of information and time given for discussion by nurses and doctors (99%), attentiveness of doctors to the patient’s history (96%), satisfactory answering of questions by the doctor (91%) and patient involvement with decisions regarding their care (95%)
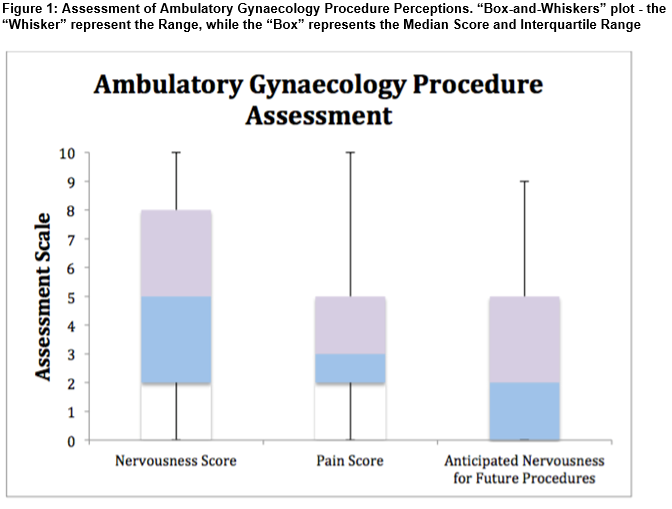
Procedure Assessment: The vast majority (97%) said that the nurse made them feel comfortable during their procedures, 96% thought the procedure was done in a way that respected their dignity, and all patients felt the staff in the clinic did their jobs well. Figure 1 presents the self-rated scales for procedure-related nervousness and pain.
Care offered following procedure: Information on what to expect in the days after the procedure was received by 86% of patients and 84% were advised on how to take care of themselves after the procedure. The majority (93%) had an explanation on what tests were done and appropriate follow-up, and 90% felt they had enough time for discussion with the doctor after the procedure.
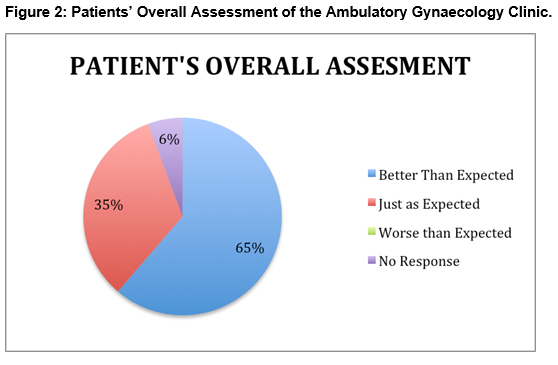
Overall Assessment: A very high proportion of patients (96%) were satisfied with the quality of care they received with 92% stating they would recommend the clinic to friends with similar problems. Preference for options other than the Ambulatory Gynaecology Clinic in the future was stated by 29%, while 58% would prefer Ambulatory Gynaecology management over other options, with 13% of patients being neutral on the issue. Figure 2 presents the overall global perception of the Ambulatory Gynaecology clinic.
Discussion
This study addresses the patient’s experience of the Ambulatory Gynaecology clinic at Mayo University Hospital. Results show a high level of patient preparedness for the procedures. The average waiting time for appointments of approximately 8 weeks was markedly shorter than average waiting times for outpatient clinics nationally. Data from the HSE-led HealthStat regarding international best practice recommends that average-waiting times for consultant-led outpatient clinics should be less than 90 days. However, a 2010 report by the Health Information & Quality Authority (HIQA), revealed that average waiting times of 16 hospitals including Mayo University Hospital exceeded this limit9.
Three quarters of patients were satisfied with the quality of information provided to prepare them for their procedures. This figure could be improved on by the provision of more tailored information depending on the procedure being performed. The majority of patients (93%) had positive views on the clinic environment; however, some patients found it difficult to locate the clinic. While a few patients complained of prolonged delays before seeing the doctor, most patients still expressed their satisfaction of the reception given to them and their entire experience at the clinic. These findings are in line with a 2001 UK study which compared women’s experience of the one-stop menstrual clinic compared with the conventional clinic with the aid of questionnaires, favouring the one-stop menstrual clinic in terms of clinic organization and continuity of care7. As a means of improving the quality of care and patient experience at our Ambulatory Gynaecology Clinic, appointment times could be reviewed and better spaced to avoid excessive waiting prior to the procedure. In addition, clearer directions could be displayed to ensure that patients are properly guided to the clinic.
While 90% of patients positively rated the quality of communication received, one in ten patients gave a negative rating for communication. It is important that all efforts be made to communicate effectively with patients in a clinical setting.
Most patients expressed a moderate level of nervousness (median score 5) during the procedure. The chaperone nurse, also known as the “vocal local”, by keeping the patients in conversation during the procedure and providing a reassuring presence, can reduce anxiety levels. The median score for nervousness levels anticipated for future procedures was 2, reflecting the positive experience of many women during the ambulatory procedure. The median pain score during procedures in this study was low, at 3 and over 90% of patients were made to feel comfortable by staff during the procedure. These findings demonstrate the acceptability of performing procedures in an ambulatory setting. All patients found the ambulatory gynaecology experience either better than expected or just as expected. No patient found the procedure to be worse than expected. These findings are consistent with results from a randomised controlled trial, in which comparably high satisfaction rates were found in outpatient versus day surgery hysteroscopy groups10. Over 80% of patients in our study were satisfied with the level of care, communication and information provided. While this is a satisfactory finding, there are aspects of the service that can still be improved upon.
Regarding patient acceptability, around a third of patients would prefer other options such as general anaesthesia, for future similar procedures. This may be explained by the fact that a quarter of women who participated in this study had not received information regarding what to expect on the day. The clinic should look to improve information content, provision and dispatch of information to the patient.
Our study shows that the quality of care provided at the clinic was highly satisfactory given that over 90% of patients were generally satisfied with their experiences and would willingly recommend the clinic to friends with similar complaints. However, a few noteworthy aspects of care could be improved upon. Issues like reducing reception waiting time, providing clearer directions to the clinic, ensuring adequate pain relief and providing adequate information on procedures can easily be addressed within a short period while issues like providing bigger waiting and changing areas would involve expansion/renovation of infrastructure and hence, would take a longer time to address.
Limitations of our study include volunteer bias as the patients who completed the questionnaire opted to do so, rather than it being mandatory for all patients. The potential bias may impact the results in either direction i.e. participants may display more or less anxiety or satisfaction or other characteristics that the actual population served. There is also the possibility that the “Hawthorne Effect” was created by performing the study in the clinic environment, as staff at the clinic were aware that patients were assessing the quality of care provided.
The patient’s journey through the Ambulatory Gynaecology clinic at Mayo University Hospital has revealed a high level of patient satisfaction in the various aspects of their care, and these findings are consistent with results from similar studies in the published literature. This approach of integrated care should be recommended as the standard approach for the management of women with abnormal uterine bleeding nationally. Important information has been gained from patient feedback through the study, which can now be used to further improve patients’ experience in their journey through the Ambulatory Gynaecology Clinic.
Acknowledgement
The authors wish to acknowledge the assistance of the Ambulatory Gynaecology Clinic administrative and clinical staff with data collection for this study.
Conflict of interest:
The authors confirm that they have no conflict of interest to declare in relation to this work.
Correspondence:
Dr Meabh Ni Bhuinneain,
Consultant Obstetrician & Gynaecologist, Department of Obstetrics and Gynaecology, Mayo University Hospital, Castlebar, Co Mayo
Email: [email protected]
References
1. Mikos T, Downes E. Ambulatory Gynaecology: What can we do? Best Prac Res Clin Obstet Gynaecol. 2005; 19: 647-661.
2. Jones K. Ambulatory Gynaecology: A new concept in the delivery of health care for women. Gynecol Surg. 2006; 3:153-156.
3. Pasternak LR, Johns, A. Ambulatory Gynaecological Surgery: risk and assessment. Best Prac Res Clin Obstet and Gynaecol. 2005; 19: 663-679.
4. Coyle D, Lowery AJ, Khan W, Waldron R, Barry K: Successful Introduction of Ring-Fenced Inpatient Surgical Beds in a General Hospital Setting. Ir Med J. 2012; 105:269-71.
5. Nuffield Institute for Health. University of Leeds and the NHS Centre for Reviews and Dissemination, University of York, Research Unit, Royal College of Physicians. The management of menorrhagia. Effective Health Care. University of Leeds, 1995.
6. Bradlow J, Coulter A, Brooks P. Patterns of Referral. Oxford, UK: Health Services Research Unit, 1992.
7. Abu JI, Habiba MA, Baker R, Halligan AW, Naftalin NJ, Hsu R, Taub N. Quantitative and qualitative assessment of women's experience of a one-stop menstrual clinic in comparison with traditional gynaecology clinics. BJOG. 2001 Sep; 108:993-9.
8. Royal College of Obstetricians and Gynaecologists. Best Practice in Outpatient Hysteroscopy. London, UK: RCOG; 2011.
9. Health Information and Quality Authority. Report and recommendation on Patient Referrals from general practice to out patient and Radiology services, including the National standard for patient referral information. Dublin, Ireland: HIQA;2011
10. Kremer C, Duffy S, Moroney M. Patient satisfaction with outpatient hysteroscopy versus day case hysteroscopy: randomised controlled trial. BMJ. 2000 Jan 29;320: 279–282.
p420