Introduction
Influenza is caused by a highly infectious RNA virus, predominantly influenza A and influenza B, which usually occurs in a seasonal pattern with epidemics in the winter months1,2. These epidemics begin abruptly, reach a peak over a 2-3 week period, and generally last for 2-3 months2. Influenza activity in Ireland increased in the community above the Irish baseline threshold of 18 per 100,000 to 84.4 per 100,000 population in January 2016, with 10 confirmed influenza cases admitted to critical care units during the week ending February 7th, 20163. The Royal College of Physicians of Ireland (RCPI), Health Service Executive (HSE) in Ireland, and Department of Health in the United Kingdom recommend that all pregnant women at any stage of pregnancy should receive the inactivated influenza vaccine. Pregnancy increases the risk of complications from influenza because of the alterations in cardiorespiratory and immunological function1,2. It is estimated that immunisation could prevent 1-2 hospitalisations per 1,000 pregnant women2.
Influenza vaccination use in pregnancy is associated with a reduction in maternal and perinatal mortality and morbidity. It is also associated with reduced rates of influenza in the infant up to 6 months of age through transfer of maternal antibodies4,5. Multiple studies have shown that the inactivated influenza vaccine can safely be given to pregnant women1,4,5. Between 2010 and 2015, there were 42 admissions with confirmed influenza in pregnancy to the National Maternity Hospital, Dublin. The total number of bed days attributed to influenza over this six-year period was 122, with a mean length of stay of 2.9 days (SD 2.1).
The annual MBRRACE-UK Confidential Enquiry report into maternal deaths presents the triennial findings of maternal mortality in the UK and Ireland. There were no maternal deaths from influenza in 2012 and 2013. This was mainly due to a low level of influenza activity in 2012 and 2013 rather than due to an increase in the uptake of vaccination among pregnant women6. There was a statistically significant decrease in deaths due to influenza, with a 67% decrease (RR 0.33, 95% CI 0.14-0.78) when comparing 2011-13 (0.38/100,000 maternal mortality rate due to influenza) with 2009-10 (1.13/100000 maternal mortality rate due to influenza); p<0.001 for trend over time1. H1N1 vaccine uptake amongst pregnant women in the UK at the time of the pandemic was low at 14.9%7.
The uptake of vaccination among all pregnant women has increased by varying degrees across the UK; in England, vaccination uptake increased from 27% in 2011-12 to 40% in 2013-14; in Scotland from 41% in 2011-12 to 49% in 2013-14; in Northern Ireland the uptake was 58% for both time-periods, and in Wales the uptake increased from 32% in 2011-12 to 71% in 2013-141,8. The rate of flu vaccination in an Irish cohort during the flu pandemic 2009-10 was 43.5%9. The estimates of flu vaccination coverage among pregnant women from 21 states in the United States of America (USA) between 2010 and 2011 was 45.6%10. The objective of this study was to determine the uptake of the annual influenza vaccine in a pregnant population and ascertain the reasons why some pregnant women did not receive it.
Methods
We conducted a prospective cohort study over a two-week period in January 2016 in the antenatal clinic in the National Maternity Hospital Dublin, a tertiary referral maternity hospital delivering over 9000 infants per year. Patients were recruited from ‘normal risk’ clinics and from the maternal medicine and diabetic service. Patient demographics, medical co-morbidities and whether or not the woman received or did not receive the influenza vaccine were recorded. In those who received the vaccination, the gestational age of receipt was documented. In those who did not receive the vaccination, the reason why not was documented. Data was analysed using SPSS version 23.0.
Results
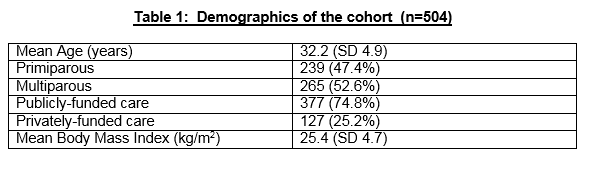
There were n=504 women studied over the 2-week period. The mean age was 32.2 years (SD 5.9). There were 239 (47.4%) primiparous women and 265 (52.6%) multiparous women. The mean body mass index (BMI) at the booking visit was 25.4 kg/m2 (SD 4.7) and the mean gestational age when studied was 31.3 weeks (SD 7.5). Three hundred and seventy-seven subjects (74.8%) attended for publicly-funded obstetric antenatal care and 25.2% (n=127) attended for privately-funded obstetric antenatal care using health insurance. Table 1 demonstrates the patient characteristics of the study. Overall, 197 (39.1%) women received the vaccine at a mean gestational age 20.9 weeks (SD 7.0, range 4-36 weeks).
Of the primiparous women, 41.8% (n=100) received the influenza vaccine. Of those who did not receive the vaccine (n=139), 35.3% (n=49) did not know that the influenza vaccine was recommended in pregnancy. Of the multiparous women, 36.6% (n=97) received the influenza vaccine. There were 16 women with asthma, 25 women with gestational diabetes, and 3 women with type 1 diabetes in the study, of which 43.8% (n=7), 60.0% (n=15) and 66.7% (n=2) respectively received the influenza vaccination. Overall, 48.1% (n=39/81) of those classified with a medical co-morbidity received the influenza vaccine. When adjusting for those without a medical co-morbidity, the overall rate of influenza vaccine uptake was 37.6% (n=159/423)
When analysed by maternal age less than 30 years (n=145), there was a 27.6% (n=40) uptake compared to a 43.7% (n=157) in those 30 years or greater (n=359), (p=0.0008). Of those less than 30 years of age who did not receive it, 38.1% (40/105) did not know it was recommended in pregnancy.When analysed by publicly-funded obstetric antenatal care compared with privately-funded obstetric antenatal care using health insurance, there was a 35.8% (135/377) uptake in public antenatal care compared with 48.8% (62/127) uptake in those under private care (p=0.01).
The uptake in those with BMI in the obese category ≥ 30kg/m2 was 40.8% (n=29/71) compared with 38.8% (n=168/433) in women with BMI < 30kg/m2 (NS).

Discussion
This prospective cohort study found that rate of uptake of the influenza vaccine in pregnancy is low at 39.1% (n=197). Within our study, 32.6% (n=164) of those who did not receive the influenza vaccine did not know that the influenza vaccine was recommended in pregnancy, and 2.9% (n=15) of this group thought that it was contraindicated in pregnancy. Furthermore, 8.8% (n=44) of these women were undecided at the time of study and 7.5% (38) had forgotten to get the influenza vaccine. There was a significantly lower uptake of the vaccine among women less than 30 years of age, and of those who did not receive it, many did not know it was recommended in pregnancy. There was also a significantly lower uptake in those who attended for publicly-funded obstetric antenatal care compared to those using private health insurance. These results are consistent with previous published Irish data9. Women with medical co-morbidities, in particular in those with asthma and diabetes, should be encouraged to receive the vaccine given the implications associated with influenza.
The uptake rates in our population are lower than those reported in the literature for the United Kingdom and the United States1,8,10. This is cause for concern. There are possible explanations for this. Pregnant women are not well informed that vaccination against influenza is recommended. Those who are informed may be unclear if they are at risk of influenza, and are unsure regarding the safety of the influenza vaccination in pregnancy. Another reason for lower uptake rates in the Republic of Ireland may be that there is a monetary charge associated with the vaccination for the majority of pregnant women.
We recommend that a more sophisticated public health campaign be put in place and that information regarding safety of the vaccination at any stage in pregnancy is promoted. Healthcare professionals, in particular, obstetricians, general practitioners and midwives have a central role to play in this communication and education. Vaccination in pregnancy is a relatively recent recommendation. As healthcare professionals gain more experience with its use and safety in pregnancy, there is likely to be an increased uptake in our population.
We recommend that the HSE considers the introduction of a free influenza vaccination programme for all pregnant women to attempt to increase rates of uptake in this group. Influenza vaccination programmes have been shown to be cost effective in studies from Europe and the USA11,12,13. Given the increased rates of influenza in the community and the associated implications for both mother and infant, it is important that we educate pregnant women regarding the risks of influenza in pregnancy and encourage this cohort in particular to be vaccinated. It is also necessary to reassure this at-risk population that the inactivated influenza is safe and recommended at any stage of pregnancy.
Correpondence: Dr David Crosby, Department of Obstetrics and Gynaecology, University College Dublin, National Maternity Hospital, Holles Street, Dublin 2.
Tel:00353-1-6372000
Email: [email protected]
Conflict of Interest
The authors have no conflict of interest to declare.
References
1. PHE, DH, NHS England (2014b). Flu Immunisation Programme 2014 to 2015
2. Royal College of Physicians of Ireland. Immunisation Guidelines for Ireland. Chapter 11 Influenza. August 2015
3. Influenza Surveillance in Ireland – Weekly Report. HPSC. February 7 2016
4. Tamma OD, Ault KA, del Rio C, Steinhoff MC, Halsey NA, Omer SB. Safety of influenza vaccination during pregnancy. Am J Obstet Gynecol. 2009; 201(6): 547-552
5. Naleway AL, Irving SA, Henninger ML, Li DK, Shifflett P, Ball S, Williams JL, Cragan J, Gee J, Thompson MG. Safety of influenza vaccination during pregnancy: A review of subsequent maternal obstetric events and findings from two recent cohort studies. Vaccine. 2014 May 30;32(26):3122-7
6. MBRRACE-UK. Saving Lives, Improving Mother’s Care. December 2015.
7. Sethi M, Pebody R. Pandemic H1N1 (swine) influenza vaccine uptake amongst patient groups in primary care in England 2009/2010. UK: Department of Health; 2010.
8. PHE, DH, NHS England (2013). Flu Immunisation Programme 2013 to 2014.
9. Cleary BJ, Rice Ú, Eogan M, Metwally N, McAuliffe F. 2009 A/H1N1 influenza vaccination in pregnancy: uptake and pregnancy outcomes - a historical cohort study. Eur J Obstet Gynecol Reprod Biol. 2014 Jul;178:163-8.
10. Seasonal influenza vaccination coverage among women who delivered a live-born infant--21 states and New York City, 2009-2010 and 2010-11 influenza seasons. MMWR 2013; 62:1001-4.
11. Beigi RH, Wiringa AE, Bailey RR, Assi TM, Lee BY. Economic value of seasonal and pandemic influenza vaccination during pregnancy. Clin Infect Dis. 2009 Dec 15;49(12):1784-92.
12. Blommaert A, Bilcke J, Vandendijck Y, Hanquet G, Hens N, Beutels P. Cost-effectiveness of seasonal influenza vaccination in pregnant women, health care workers and persons with underlying illnesses in Belgium. 2014 Oct 21;32(46):6075-83.
13. Roberts S, Hollier LM, Sheffield J, Laibl V, Wendel GD Jr. Cost-effectiveness of universal influenza vaccination in a pregnant population. Obstet Gynecol. 2006 Jun;107(6):1323-9.
p449