Neonatal Thyroid Function: Test First, Think Second?
L E Geraghty, M J O’Grady
Department of Paediatrics, Midland Regional Hospital, Mullingar, Co. Westmeath
The prevalence of autoimmune thyroid disease is up to 2.5% amongst pregnant women. However trans-placental passage of thyroid peroxidase (TPO) and thyroglobulin antibodies is not harmful to the foetus. Conversely, thyroid-stimulating hormone (TSH) receptor-stimulating antibodies can cause foetal and neonatal thyrotoxicosis in 1-10% of cases of maternal Graves’ disease, and TSH receptor-blocking antibodies can lead to transient congenital hypothyroidism (CH). The incidence of the latter disorder is 1:180,000 normal infants, or approximately 2% of babies with CH. In 93% of such infants, thyroid function tests (TFTs) normalise by day 151.
Newborn screening for primary CH detects elevated bloodspot TSH and the value of supplemental venous TFTs in infants of mothers with Hashimoto’s thyroiditis has been questioned2. Using a standardised proforma, we conducted a telephone survey of all 19 maternity units in June 2015 regarding testing policies, indications for and timing of postnatal TFTs.
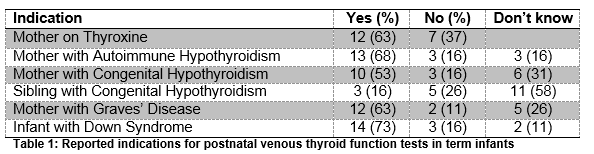
Responses were received from all 19 maternity units. Five (26%) had a formal policy regarding TFTs in term neonates. Reported indications for postnatal venous sampling are outlined in Table 1. Three (16%) requested autoantibodies at the time of sampling.
The practice of supplemental testing of infants born to mothers with autoimmune hypothyroidism occurs in centres which collectively deliver between 73-82% of all infants born in the Republic of Ireland. We estimate that approximately 1,500 infants annually undergo duplicate testing, for a condition, which will affect one infant in Ireland every three years, and is detectable using bloodspot TSH. Thirty-seven percent of centres test on or before day 5; up to 28% of TFTs performed in infants of mothers with autoimmune thyroid disease will be mildly abnormal at this time resulting in further testing3. Forty-seven percent of centres test between day 5-10, having already had bloodspot TSH measurement. The remainder were tested beyond the optimal window for initiation of thyroxine in infants with CH.
Neonatal thyrotoxicosis is not detected on bloodspot TSH-based newborn screening. Its presence can also be masked initially by transplacental passage of maternal antithyroid drugs. Risk is greater when maternal TSH receptor antibodies between 24-28 weeks gestation are three times the upper limit of normal4. The fact that less than two-thirds of units appropriately undertake testing of infants where there is maternal thyrotoxicosis is a concerning finding as severe neonatal Graves’ disease can be fatal if untreated.
Laboratory testing is unnecessary in infants of mothers with Hashimoto’s thyroiditis or mothers receiving thyroxine (unless as a result of treatment for Graves’ disease). They are also unnecessary in infants with Down syndrome, and are not recommended in national guidelines. Infants at high risk of neonatal Graves’ disease (early third trimester maternal TSH receptor antibody 3 times the upper limit of normal or unknown; antithyroid drug use in the third trimester; evidence of foetal thyrotoxicosis) should be examined for evidence of thyrotoxicosis and should have TFTs, T3 and TSH receptor antibodies performed on postnatal day 2-5. All mothers with Graves’ disease should be advised of the signs and symptoms of thyrotoxicosis in their infants who should be reviewed again on postnatal day 10 for bloods and clinical exam.
Conflict of Interest:
The authors have no conflicts of interest to declare
Correspondence
Dr Michael O’Grady, Department of Paediatrics, Midland Regional Hospital, Mullingar, Co. Westmeath
Email: [email protected]
References
- Brown RS, Bellisario RL, Botero D, Fournier L, Abrams CA, Cowger ML, David R, Fort P, Richman RA. Incidence of transient congenital hypothyroidism due to maternal thyrotropin receptor-blocking antibodies in over one million babies. J Clin Endocrinol Metab. 1996 Mar; 81(3):1147-51.
- Ogilvy-Stuart AL. Neonatal thyroid disorders. Arch Dis Child Fetal Neonatal Ed. 2002;87(3):F165-71
- Rovelli R, Vigone MC, Giovanettoni C, Passoni A, Maina L, Corrias A, Corbetta C, Mosca F, Chiumello G, Weber G. Newborn of mothers affected by autoimmune thyroiditis: the importance of thyroid function monitoring in the first months of life. Ital J Pediatr. 2010 Mar 10;36:24.
- Stagnaro-Green A, Abalovich M, Alexander E, Azizi F, Mestman J, Negro R, Nixon A, Pearce EN, Soldin OP, Sullivan S, Wiersinga W; American Thyroid Association Taskforce on Thyroid Disease During Pregnancy and Postpartum. Guidelines of the American Thyroid Association for the diagnosis and management of thyroid disease during pregnancy and postpartum. Thyroid. 2011 Oct;21(10):1081-125.
p460