Introduction
In 2011, the Programme for Government committed to end long-term homelessness and the need to sleep rough. These goals were to be achieved by building on the 2008 National Strategy entitled The Way Home: A Strategy to Address Adult Homelessness in Ireland1. A ‘housing first’ approach was promised in which the provision of suitable, affordable accommodation for people at risk of homelessness was to be prioritised. In 2013, the Government, in their Homeless Policy Statement, promised to end long-term homelessness by 20162.The situation has deteriorated since 2013. The Dublin Region Homeless Executive (DRHE) reported that 4,006 adults accessed emergency accommodation in the third quarter (Q3) of 20163. Of these, 17% were presenting for the first time - an average of 7.3 new people presenting per day over that period. The number of individuals accessing emergency accommodation increased by 20% in the 12 months to Q3 2016 and by 63% over the past two years3. In November 2016 it was reported that there were over one thousand families and over two thousand children homeless in Dublin – a 44% increase in just one year4.
The first assessment of the health of the homeless population in Dublin was conducted in 19975. In 2005 and 2013, two further cross-sectional surveys used similar study instruments and sampling strategies to examine the health of the homeless population6, 7. The proportion of respondents who had become homeless primarily as a result of drug and/or alcohol addiction increased from 24% (n=84/353) in the 1997 study to 38% (n=203/536) in the 2013 study. Similarly, the proportion of the study cohorts who had ever used drugs increased from 29% in 1997 to almost 80% in 2013. There was also a large increase in the proportion of respondents who identified themselves as active drug users, increasing from 23% of the study cohort in 2005 to 54% in 2013. While data on drug-related deaths in the homeless has not previously been published in Ireland, international data suggests that rates of drug-related death are very substantially increased in the homeless versus fixed residence population8. The proportion of respondents in the aforementioned Irish surveys with at least one physical or mental ill-health diagnosis increased from 68% in the 1997 cohort to 90% in 2013. Furthermore, an analysis of emergency in-patient hospitalisations among those of ‘no fixed abode’ (NFA) in Ireland between 2005 and 2014 reported that 57% had a mental/behavioural diagnosis9. In the 2013 survey, over 50% of respondents (32% in 1997) reported a diagnosis of depression, 29% of respondents reported suicidal ideation in the previous six months and more than one third had previously attempted suicide.7 Separately, an analysis of data from the National Self-Harm Registry Ireland reported that, between 2006 and 2011, the number of self-harm presentations by homeless people increased from 285 to 473, representing an overall increase of 66%. This was significantly higher compared to the 22.6% among those with a fixed residence10.
It is clear, therefore, that a substantial proportion of people who are homeless in Ireland today have ended up – and remain - in that position because of ill-health and addiction. Along with the survey and other data discussed above, a number of papers have also been published on the primary care needs of those who are homeless in Ireland6, 11-13 and the links between homelessness, addiction and perceived quality of life14. This work aims to build on this evidence by collating data on methadone use, drug-related deaths and emergency department presentations due to self-harm in people categorised as being of NFA or homeless from prospectively collected databases, and to discuss the implications of this evidence for those tasked with providing services to this vulnerable population.
Methods
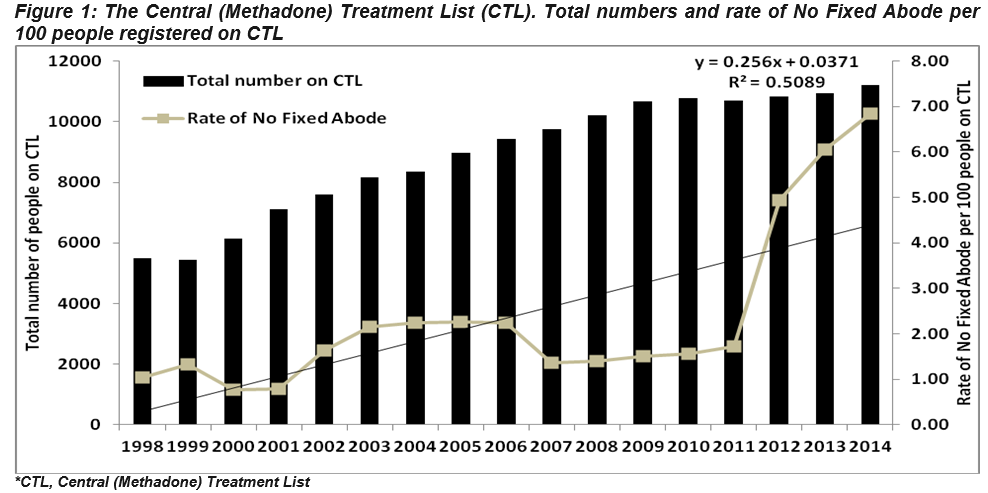
Three data sources were used to assess the health of the homeless population in Ireland. The Central (Methadone) Treatment List (CTL) is a register of all people prescribed methadone for the treatment of opiate addiction in Ireland. The total number of people on the CTL and the number and proportion of those registered as homeless between 1998 and 2014 was reviewed. The National Self-Harm Registry Ireland is a national system of population monitoring for the occurrence of deliberate self-harm and has national coverage of self-harm presentations to hospital emergency departments15. The total number of cases recorded by the Registry between 2008 and 2014 was examined, together with the number and proportion of those cases registered as being of NFA. The National Drug-Related Deaths Index (NDRDI) is a census of deaths by drug and/or alcohol poisoning, and deaths due to all causes among drug users and among alcohol dependent persons in Ireland. The total number of deaths recorded by the NDRDI and the number and proportion of those deaths in people registered as homeless between 2004 and 2013 was examined.
Results
Central (Methadone) Treatment List (CTL)
The total number of people on the CTL nationally increased from 5,498 in 1998 to over 11,000 in 2014 (Figure 1). Between 1998 and 2014, the percentage on the CTL who were registered as being of NFA increased from one percent (57/5,498) to 7% (766/11,206). It increased from two percent (184/10,711) to 7% between 2011 and 2014 alone (Figure 1). This data is at the national level and, while it includes Dublin, individual data for Dublin was not available for the time period examined. However, in May 2015 a total national figure of 664 persons of no fixed abode were recorded on the CTL, of which 534 (80.4%) were in Dublin.
National Self-Harm Registry Ireland
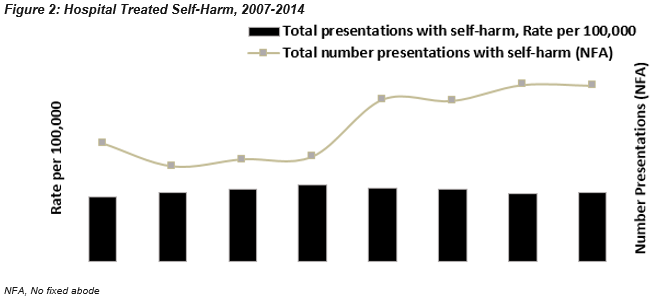
Nationally, the rate of self-harm in the population as a whole in Ireland has increased since 2007. The largest increase was observed between 2007 and 2010, where the overall rate increased from 188 to 223 per 100,000 (+19%). Despite decreases in the rate of self-harm in recent years, the rate in 2014 was still 6% higher than that recorded in 2007 (+14% for men, one percent for women) (Figure 2). On average, approximately 11,000 presentations are recorded annually by the Registry, with approximately 500 of these registered as being of NFA (Figure 2). The proportion of presentations recorded by the Registry in people who were of NFA increased from three percent in 2007 to 5% in 2014. The absolute number of presentations increased by 49% between 2007 (n=344) and 2014 (n=514) (Figure 2). This increase was more pronounced among women (+68%).
Figure 2: Hospital Treated Self-Harm, 2007-2014
The number of drug- and alcohol-related deaths recorded nationally increased by 57% from 2004 (n=933) to 2013 (n=1,465), inclusive. Over that time period there were 494 deaths nationally of individuals known to be homeless (Figure 3). Almost two thirds (65%, n=320) of these deaths were in Dublin.
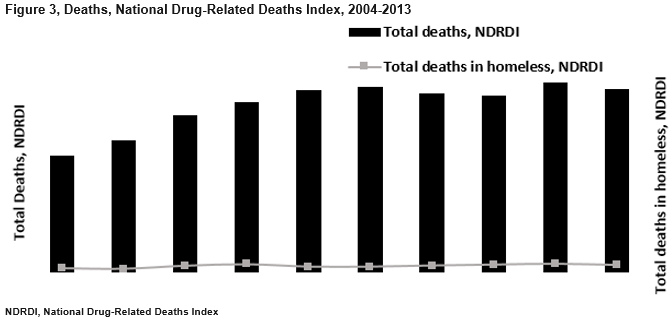
The number of drug- and alcohol-related deaths among those who resided in Dublin increased by 41% from 2004 (n=419) to 2013 (n=590). The number of deaths amongst those identified as homeless and who died in Dublin fluctuated over the time period with an overall upward trend. Twenty two (54%) of the 47 deaths in Dublin in 2013, in those identified as homeless, were directly attributable to poisoning. Of these, 17 (77%) involved polydrug use. Opiates were implicated in 21 (95%) of the deaths.
Discussion
Despite an increase in the proportion of the homeless population with medical cards and the development and roll-out of Safetynet and other primary care services for the homeless, the health needs of this population have remained substantial over the past twenty years6, 7, 9, 12. The evidence presented here from the National Self-Harm Registry Ireland suggests that the incidence of self-harm has increased within the homeless population in recent years. This evidence correlates with a previous analysis of data from the Registry which reported that over the period 2006-2011, the risk of self-harm among people who are homeless was 22 times higher compared to those with a fixed residence10. It also supports the results of work by Dunne and colleagues in 2012 in which users of the mental ill-health service for homeless people in Cork (n=54) were profiled; users of this service were more likely to have a history of self-harm (54% vs. 21%) when compared with those attending a General Adult Service. In addition, there was a significantly higher prevalence of schizophrenia (50% vs. 34%), personality disorder (37% vs. 11%) and substance dependence (74% vs. 19%) in the homeless service users.16
Evidence across a range of parameters suggests that prevention and treatment of drug and alcohol addiction within the homeless population has not been adequately addressed over the past twenty years. Almost 40% of this population now identify drug and/or alcohol problems as the primary cause of their homelessness and 80% of those who are homeless have used drugs7. In contrast, just 27% of the general population in Ireland have reported ever taking drugs17. In addition, the proportion of the homeless population who are current drug users appears to have increased dramatically over the past ten years. These findings are reflected in the data provided by the CTL with a substantial increase seen in the proportion of people who are homeless recorded on this Register. This inter-play between homelessness and drug use was highlighted in Ireland in 2015 during the investigation of an outbreak of HIV subtype B among people who inject drugs (PWID) in Dublin. Between January 2014 and September 2015, 38 new cases were reported; all of the females (n=16) and 13 of the 20 males with information available were registered with homeless services18.
Although the 2008 National Strategy on homelessness recognised that “homeless services have traditionally developed in response to urgent needs and in an uncoordinated manner” and that this approach was suboptimal1, there remains a lack of an overarching plan with respect to the health of homeless people in Ireland. The result has been the introduction of a range of measures, including the provision of additional emergency accommodation and measures to provide rent certainty which, while welcome and needed, were not targeted specifically at the health needs of those at risk of, or currently experiencing, homelessness. Similarly, while a number of public health harm reduction policies (i.e. the provision of medically supervised safer injecting rooms, decriminalisation of drug use) have been implemented or are currently being considered in Ireland – and which could potentially have significant impact on the health of our homeless population - none have been developed with the homeless population specifically in mind.
There are a number of important limitations to this work. Firstly, the evidence presented from the CTL, the National Self-Harm Registry Ireland and NDRDI does not take account of the total number of people who are homeless in Ireland; hence neither incidence nor prevalence can be calculated and the increases in the numbers of homeless recorded in these registers should not be taken to represent proportionate increases in methadone use, self-harm or drug-related deaths in the homeless population as a whole. However, the absolute increases seen nevertheless represent a significant burden on our health and social care services and are important findings in their own right. Secondly, the data presented here relates to those recorded as ‘no fixed abode’ and/or ‘homeless’; it is possible that the ‘no fixed abode’ categorisation only captured those accommodated in temporary emergency accommodation (one-night only) and those who were ‘roofless’ or rough-sleeping, and that those in supported temporary accommodation (typically for six months with case management) were not included,9 and hence the numbers affected by homelessness may have been underestimated.
In conclusion, while there are a number of important caveats, the data presented here from relevant national registers, together with the trends seen in published surveys in relation to physical and mental ill-health, risk behaviours and addiction, suggest a care system which is failing one of its most vulnerable groups. Addressing these issues will require a multi-faceted approach. While a housing-led strategy is required and there is an urgent need to build more houses and address rising rents, there is also an urgent need to adequately resource and coordinate those services which aim to address all of the other factors (social and health inequalities, mental ill-health and addiction) which lead people into – and prevent them exiting from – homelessness.
Conflicts of Interest
None to declare
Funding
No funding
Acknowledgements:
The authors wish to thank Professor Joe Barry, Professor of Population Health Medicine, Trinity College Dublin, for his support in the preparation of this manuscript. They also wish to acknowledge the work of those involved in the collation of data for the Central (Methadone) Treatment List (CTL), the National Self-Harm Registry Ireland and the National Drug-Related Deaths Index (NDRDI).
Correspondence:
Dr. Ronan Glynn, Department of Public Health East, Dr. Steevens’ Hospital, Dublin 8, Ireland.
Tel: 00353851996008
Email: [email protected]
References
1. Department of the Environment. The way home: a strategy to address adult homelessness in Ireland, 2008-2013. Dublin, 2008.
2. Department of the Environment. Government Homeless Policy Statement. Dublin, 2013.
3. Performance Report relating to the Protocol Governing Delegation of Section 10 Funding for Homeless Services to Dublin City Council. Dublin: Dublin Region Homeless Executive; 2016.
4. Dublin Region - families who are homeless. Infographic. Dublin: Dublin Region Homeless Executive; 2016.
5. Holohan T. Health status, health service utilisation and barriers to health service utilisation among the adult homeless population in Dublin. Dublin: Eastern Health Board; 1997.
6. O'Carroll A, O'Reilly F. Health of the homeless in Dublin: has anything changed in the context of Ireland's economic boom? Eur J Public Health. 2008;18(5):448-53.
7. O' Reilly F, Barror S, Hannigan A, Scriver S, Ruane L, MacFarlane A, O'Carroll A. Homelessness - An unhealthy state. Health status, risk behaviours and service utilisation among homeless people in two Irish cities. Dublin: The Partnership for Health Equity.; 2015.
8. Hwang SW, Wilkins R, Tjepkema M, O'Campo PJ, Dunn JR. Mortality among residents of shelters, rooming houses, and hotels in Canada: 11 year follow-up study. Bmj. 2009;339:b4036.
9. O'Farrell A, Evans DS, Allen M. The Epidemiology of Emergency In-Patient Hospitalisations Among Those with 'No Fixed Abode' (Homeless) 2005-2014: What Lessons Can Be Learnt. Ir Med J. 2016;109(9):464.
10. Arensman E, Mhuircheartaigh E, Corcoran P. Briefing - Self harm and suicide among homeless people. Cork: National Suicide Research Foundation (NSRF); 2014.
11. O'Donnell P, Tierney E, O'Carroll A, Nurse D, MacFarlane A. Exploring levers and barriers to accessing primary care for marginalised groups and identifying their priorities for primary care provision: a participatory learning and action research study. Int J Equity Health. 2016;15(1):197.
12. O'Carroll A, Irving N, O'Neill J, Flanagan E. A review of a GP registrar-run mobile health clinic for homeless people. Ir J Med Sci. 2016.
13. Keogh C, O'Brien KK, Hoban A, O'Carroll A, Fahey T. Health and use of health services of people who are homeless and at risk of homelessness who receive free primary health care in Dublin. BMC Health Serv Res. 2015;15:58.
14. O'Brien KK, Schuttke A, Alhakeem A, Donnelly-Swift E, Keogh C, O'Carroll A, O' Sullivan K, Galvin R, Fahey T. Health, perceived quality of life and health services use among homeless illicit drug users. Drug Alcohol Depend. 2015;154:139-45.
15. Griffin E, Arensman E, Corcoran P, Dillion C, Williamson P, Perry I. National Self-Harm Registry Ireland Annual Report, 2014. Cork: National Suicide Research Foundation; 2015.
16. Dunne E, Duggan M, O'Mahony J. Mental health services for homeless: patient profile and factors associated with suicide and homicide. Ir Med J. 2012;105(3):71-2, 4.
17. National Advisory Committee on Drugs and Alcohol. Drug use in Ireland and Northern Ireland, 2010/11. Dublin, 2011. p. 28.
18. Giese C, Igoe D, Gibbons Z, Hurley C, Stokes S, McNamara S, Ennis O, O'Donnell K, Keenan E, De Gascun C, Lyons F, Ward M, Danis K, Glynn R, Waters A, Fitzgerald M. Injection of new psychoactive substance snow blow associated with recently acquired HIV infections among homeless people who inject drugs in Dublin, Ireland, 2015. Euro Surveill. 2015;20(40).
(P631)