Travel health cardiovascular risks
Certain aspects of the travel experience are likely to place heavier demands on the cardiovascular system. These include the stress of navigating airports, carrying heavy luggage, and dealing with the inevitable queues, security checks, and unpredictable flight delays. Long-haul flights in the hypoxic environment of a commercial aircraft, disorientation and security concerns at the destination, combined with the effects of jet lag all exact a toll on the traveller with heart disease. Travel to extremely cold climates may precipitate acute coronary syndromes3, while excessive heat stress can lead to postural hypotension, especially in patients taking antihypertensive agents, including diuretics. The modern leisure traveller may participate in adventure activities such as sky-diving without giving due consideration to their effects on the cardiovascular system.
Pre-travel preparation
Travel insurance
Travellers with CVD should declare their medical histories to their travel insurance company and ensure that their policy covers their medical care in the event of acute illness occurring during their planned activities abroad. Insurance policies should cover local medical costs as well as expensive medical evacuation or repatriation to another country or the patient’s home country for definitive medical care4. Where possible, it is better to travel with a companion and to communicate one’s medical history to this person. Copies of their medical summary, baseline electrocardiogram and prescriptions should be transported in hand luggage.
Fitness-to-travel evaluation
Published recommendations are available to guide decisions about fitness to fly in patients with cardiovascular disease5, cyanotic congenital heart disease6, and heart failure7 and the traveller may need additional assessments to determine their capacity to travel, including a treadmill exercise stress test or echocardiogram. In some cases, especially where the patient has had a recent hospital admission or change in cardiac medications, it may be better to postpone international travel until the condition has stabilised.
Travel vaccinations
The traveller with CVD should receive standard pre-travel health advice, tailored for the destinations involved, including food and water precautions, insect bite avoidance, and animal bite wound care in rabies endemic countries. Routine, recommended and required (e.g. yellow fever) travel vaccinations should be administered in the context of a travel health consultation. Additional vaccines to be considered in the CVD patient include influenza vaccine, pneumococcal vaccine, and hepatitis B vaccine. Where the traveller is taking warfarin as thromboprophylaxis, the international normalised ratio (INR) should be known before the administration of intramuscular vaccine injections.
Malaria chemoprophylaxis
A comprehensive risk assessment of the traveller’s likely exposure to mosquito bites in malaria endemic areas should be performed. Where malaria chemoprophylaxis is indicated, mefloquine should be avoided in patients with heart disease, and atovaquone-proguanil or doxycycline used instead. Written guidance should be provided on how to take the medication as well as the steps to take in the event of a fever upon return from their travels. Drug-drug interactions between anti-malarial medication and cardiac medications should be discussed with the patient’s cardiologist.
Health issues during travel
Air travel considerations
The traveller with CVD should discuss the need for in-flight supplemental oxygen with their general practitioner and with the airline company at least 2 weeks in advance of travel. They should also request wheelchair assistance at airports if the transfer demands from the check-in desks to their gate exceed their maximum exercise tolerance. A letter from their general practitioner may be required to obtain supplemental oxygen or extra assistance, and this letter should also be presented at the airport security station. It is important to keep well hydrated during the flight and to avoid caffeinated or alcoholic beverages; the traveller should be encouraged to walk frequently down the cabin aisle, in order to reduce the risk of travellers’ venous thrombosis. Where there is no evidence of peripheral arterial disease, it is reasonable for the traveller with heart disease to wear below knee compression flight socks for the duration of their journey.
Travel with cardiac devices
Implanted cardiac devices such as permanent pacemakers and cardioverter-defibrillators facilitate travel for many patients with heart disease. The patient should not travel by air within 2 weeks of successful drainage of a procedure-related pneumothorax. Difficulties at airport screening may be avoided by declaring the presence of the device, and providing the screening personnel with a device card and physician letter. The manufacturer’s card should display the device brand and identification number. The security officer may perform a pat-down search instead and avoid passing over the device with a hand-held security wand5. The traveller should have access to manufacturer contact information during travel in case of apparent device malfunction.
Medication issues and travel
All medications should be transported in their original pharmacy-labelled containers and in double the quantities required for the trip. Medications must not be packed in the luggage hold during the flight. The use of sedative hypnotics should be strongly discouraged as they will impair mobilisation efforts during the flight. Medications should be taken at the destination local time to avoid confusion. For long-term or expatriate travellers, prior contact should be made with a local physician or pharmacist to ensure that an equivalent drug is available in the host jurisdiction. Some medications may degrade with exposure to sunlight so all drugs should be stored in a cool, dry place. With disruption of one’s normal daily routine, patient medication adherence may be compromised, and the traveller should use day-labelled blister packs to ensure compliance.
Warfarin anticoagulation during longer trips will require access to a reliable INR monitoring clinic or calibrated point of care device. Where the INR is unstable prior to prolonged travel, it may be possible to convert the patient to a novel oral anticoagulant to avoid the need for monitoring8. The anticoagulated patient should be careful not to markedly increase the amount of dietary vitamin K to avoid the risk of developing a subtherapeutic INR9. The risk of dangerous bleeding from traumatic physical injury should be borne in mind when considering adventure pursuits where falls are a risk.
Travel risk behaviour
Travelling hypertensive patients and patients with chronic heart failure should minimise salt intake in their diets abroad. They should also avoid exposure to thermal extremes. Travel to high altitude presents particular risks for decompensation of heart failure or precipitation of angina symptoms10, and the patient should be counselled on these risks. Table 1 summarises the main considerations for the cardiac patient at altitude, but additional information should be sought where acetazolamide chemoprophylaxis of acute mountain sickness is considered11. Travel can be sedentary and all cardiac patients should continue to engage in moderate intensity physical activity but avoid unaccustomed exertion and a frantic travel itinerary. Alcohol intake should be moderate, and strict food and water safety advice should be followed throughout the trip to avoid travellers’ diarrhoea.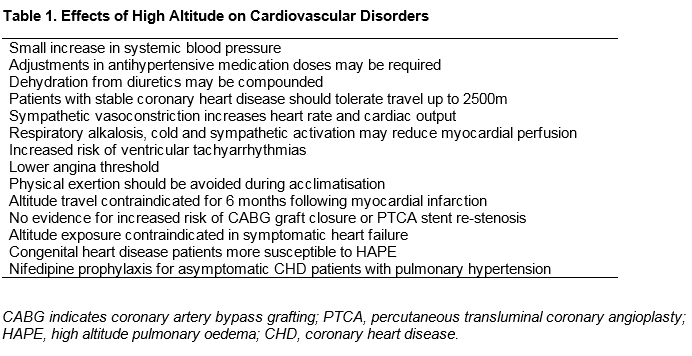
Accessing medical care abroad
Healthcare resources in many popular tourist destinations in developing countries are inferior to the traveller’s domestic medical care, and the ill traveller may find it difficult to access appropriate medical care in an emergency, especially in a remote wilderness setting. A MedicAlert® bracelet may be critically important in the event of a sudden collapse in an unfamiliar environment. The CVD traveller should be familiar with how to summon emergency medical care and should carry a list of local English-speaking physicians12.
Post-travel considerations
Febrile illness, rash, diarrhoea, and eosinophilia are the most common clinical presentations of disease in the returned traveller. The failure to obtain a travel history in an ill returned traveller can lead to potentially fatal diagnostic delay where a traveller has developed a tropical infectious disease13. The intending traveller should be advised to seek immediate medical help in the event of a fever occurring up to 6 months after returning from a malaria area. Travel to tropical regions may itself cause heart disease, including Chagas disease, which may present to a general practitioner with shortness of breath secondary to dilated cardiomyopathy14.
Conclusion
The majority of patients with heart disease will find their travels rewarding and beneficial to their health and wellbeing. Patients should be encouraged to travel with due attention to travel health risks and precautions. Close cooperation between the travelling patient, the general practitioner, and cardiologist will help to promote safe and healthy international travel.
Competing interests
None.
Correspondence: Dr. Gerard Flaherty, MD, School of Medicine, National University of Ireland, Galway, Ireland. E-mail [email protected]. Telephone +353-91495469. Fax +353-91494540.
References
1. World Tourism Organization. UNWTO Annual Report 2014. Available at: http://www2.unwto.org/annualreport2014 [Accessed 10 June 2016].
2. Wieten RW, Van der Schalie RM, Visser BJ, Grobusch MP, van Vugt M. Risk factors and pre-travel healthcare of international travellers attending a Dutch travel clinic: a cross-sectional analysis. Travel Med Infect Dis 2014;12:511-524.
3. Klug G, Schenk S, Dörler J, Mayr A, Haubner BJ, Alber H, Schächinger V, Pachinger O, Metzler B. Occurrence of acute myocardial infarction in winter tourists: data from a retrospective questionnaire. Clin Res Cardiol 2011;100:669-674.
4. Leggat PA, Griffiths R, Leggat FW. Emergency assistance provided abroad to insured travellers from Australia. Travel Med Infect Dis 2005;3:9-17.
5. Smith D, Toff W, Joy M, Dowdall N, Johnston R, Clark L, Gibbs S, Boon N, Hackett D, Aps C, Anderson M, Cleland J. Fitness to fly for passengers with cardiovascular disease. Heart 2010;96:1-16.
.6. Harinck E, Hutter PA, Hoorntje TM, Simons M, Benatar AA, Fischer JC, de Bruijn D, Meijboom EJ. Air travel and adults with cyanotic congenital heart disease. Circulation 1996;93:272-276.
7. Ingle L, Hobkirk J, Damy T, Nabb S, Clark AL, Cleland JG. Experiences of air travel in patients with heart failure. Int J Cardiol 2012;158:66-70.
8. Ringwald J, Grauer M, Eckstein R, Jelinek T. The place of new oral anticoagulants in travel medicine. J Travel Med 2014;12:7-19.
9. Fiumara K, Goldhaber SZ. A patient’s guide to taking coumadin/warfarin. Circulation 2009;119:e220-e222.
10. Mieske K, Flaherty G, O’Brien T. Journeys to high altitude – risks and recommendations for travellers with preexisting medical conditions. J Travel Med 2010;17:48-62.
11. Flaherty GT, Kennedy KM. Preparing patients for travel to high altitude: advice on travel health and chemoprophylaxis. Br J Gen Pract 2016;66:e62-64.
12. International Association for Medical Assistance to Travellers. 2016. Available at: https://www.iamat.org/ [Accessed 10 June 2016].
13. Gately R, Economos H, Fleming C, Flaherty G. Obtaining a reliable travel history from ill returned travellers. Travel Med Infect Dis 2015;13:342-43.
14. Kalil-Filho R. Globalization of Chagas disease burden and new treatment perspectives. J Am Coll Cardiol 2015;66:1190-2.
P486