CP Hawkes1,2, SM O’Connell3
1The National Children’s Research Centre, Crumlin, Dublin 12
2Division of Endocrinology and Diabetes, The Children’s Hospital of Philadelphia, USA
3Department of Paediatrics and Child Health, Cork University Hospital, Wilton, Cork
Abstract
Many countries have established regulations regarding growth hormone (GH) treatment in children, to standardise care and control cost. In this study, we describe current practice in Ireland surrounding child measurement and the approach to diagnosis of GH deficiency. A questionnaire was sent to 139 paediatricians in Ireland and 35 (9 paediatric endocrinologists) responded. Only 13 (37.1%) use the recommended 2-person technique for measuring children under 2. Amongst GH prescribers, there were a variety of GH Stimulation Tests used, sex steroid priming was used by 8 (80%) and the general cut-off for a passed test was consistent (7 ng/ml). Brand rotation (n=5, 50%) and cost (n=3, 30%) were the most common criteria for deciding the formulation of GH prescribed. We recommend that departments review their child measurement technique and equipment. We also advise the establishment of national guidelines for the use of GH, and a prospective registry for GH treated children.
Introduction
Short stature (SS) can be the presenting feature of a wide range of medical conditions including chronic illness, psychosocial deprivation, syndromic, skeletal and endocrine disorders1. Growth hormone deficiency (GHD) (primary, secondary or idiopathic) is a less common cause of faltering growth but early diagnosis and treatment can optimise final adult height2. Hence, the diagnosis and management of pediatric GHD is primarily focused on timely detection and management of growth hormone (GH) responsive SS. Variation in practice has been reported across all areas in the evaluation of children with potential GHD in Europe and the United States3,4. At the level of primary care, inaccurate measurement is a source of error. Factors contributing to this include incorrect equipment or technique, and child movement5. Inaccurate height measurement can lead to inappropriate specialist referral and parental anxiety. Serial measurements at least six months apart can be helpful6 and the provision of structured auxological training can improve the measurement accuracy7. Following referral to a paediatric endocrinologist, the recommended evaluation includes the review of growth patterns, exclusion of treatable causes of aberrant growth, measurement of insulin-like growth factor-I (IGF-I) and, if indicated, confirmatory growth hormone stimulation test (GHST)8. The GHST has poor specificity for diagnosing GHD, and up to half of normal children will be characterised as having GHD by this test 10. Arbitrary cut-off values are used to determine if a child ACHIEVES A SUFFICIENT GH CONCENTRATION achieves, despite little consideration being given to the wide variation between assays used to measure GH11 and the different agents used in GHSTs12. In addition, sex steroids may potentiate GH secretion during a GHST13 but priming with sex steroids in pre-pubertal children is not standardised.
Once the decision is made to treat a child with a daily subcutaneous injection of GH, factors determining the formulation prescribed are not known. The cost of GH is up to €50,000 per patient per year14, with significant variation between the cost of different brands of GH available in Ireland. Following final height attainment, the current recommendations are to re-evaluate the GH axis at least one month after the discontinuation of treatment, except for children with structural pituitary defects or other exceptions15. In those with persistent GHD, there are benefits to body composition, bone health and quality of life with GH replacement in adulthood16. In order to address variations in practice and the significant cost of GH therapy, many countries have established policies surrounding its use17. Ireland does not currently have an established policy regulating GH prescribing in paediatric patients. The aim of this study was to determine if the variation in practice described in other countries also exists in Ireland.
Methods
Following review of variations in practice reported elsewhere, we developed a questionnaire targeted to the four stages of the evaluation of children with possible GHD: growth evaluation in general paediatric care; diagnostic evaluation of GHD; prescribing of GH; and discontinuation of therapy. This questionnaire was developed using Survey Monkey (CA, United States), and was approved by the Clinical Research Ethics Committee of the Cork Teaching Hospitals. This was sent to all practicing Consultant Paediatricians in Ireland, sourced through the Faculty of Paediatrics in November 2013. One follow up email was sent to non-responders 1 month later. Physicians completing this questionnaire initially answered questions regarding demographics and whether or not they prescribed GH. Those who prescribe GH were subsequently asked questions regarding GH testing, treatment and discontinuation.
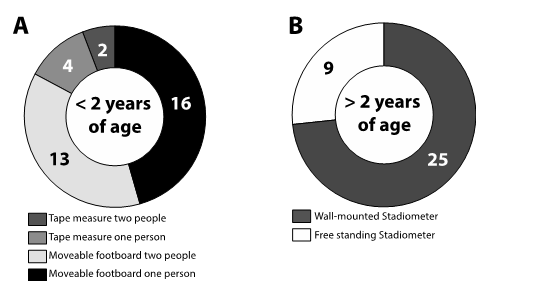
Figure 1: Methods and equipment used for measuring children less than 2 years of age (A) and over 2 years of age (B).
Results
Of the 139 paediatricians who received the questionnaire, 35 (25.2%) responded, including 1 neonatologist, and 34 general paediatricians (of whom 9 reported that they completed subspecialty training in paediatric endocrinology).
Growth Assessment
The most commonly used growth charts were the World Health Organisation Growth Charts, as recommended by the Health Service Executive in Ireland (n=32, 91.4%).The Child Growth Foundation Charts (n=5, 14.2%) and Hoey 1987 Charts (n=6, 17.1%) were also used. One quarter of respondents had a nurse trained specifically in auxology in their clinic. Only 13 (37.1%) reported measuring children less than 2 years of age using the recommended technique of 2 people measuring using a movable footboard18. For older children, 73.5% (n=25) use a stadiometer that is fixed to the wall and calibrated daily (Figure 1).
Growth Hormone Deficiency Evaluation
Ten respondents reported that they prescribe GH and were included in the remainder of the questionnaire. Criteria for starting GH treatment were variable. All agreed that poor height velocity (HV) and low IGF-I were required. Four required the patient to fail two GHSTs performed on separate days. One required the patient to fail one of two GHSTs performed on separate days. The remaining half of respondents performed only one GHST, but practice varied depending on the clinical features. The glucagon stimulation test was the most common test used (90%, n=9). Insulin tolerance test (80%, n=8), arginine (30%, n=3) and clonidine (10%, n=1) were also used. Two providers stated that glucagon is used under 4 years of age, while insulin tolerance test is used in older children. Nine respondents used a cut off of <7 ng/ml as the response required to pass the stimulation test, while one used a cut off of 6.7 ng/ml. Four would sometimes prescribe GH inpatients who pass stimulation testing if clinical suspicion indicated.
Eight respondents (80%) administered sex steroids in pre-pubertal children undergoing GHST. Criteria used for this were bone age >10 years with no clinical signs of puberty (n=7, 87.5%) or pre-pubertal children with a chronological age >12years (n=1, 12.5%). Medication and dose used for boys was Sustanon (Organon Pharmaceuticals, NJ, USA) 100 mg three days pre-test (n=7, 87.5%) or 50 mg one week pre-test (n=1, 12.5%). Fewer respondents (n=5, 50%) provided sex steroids to girls and more variation existed in doses used. Ethinylestradiol 10 mcg for three days pre-test was used by three respondents (60%), 20 mcg daily for a week was used by one and 5 mcg daily for three days was used by another. Criteria for treating suspected GHD in a neonate with other pituitary hormone deficits were low GH during hypoglycemia (n=7, 70%), low IGF-I (n=3, 30%), stimulation testing (n=2, 20%). No respondent used random GH levels to diagnose GHD in this population.
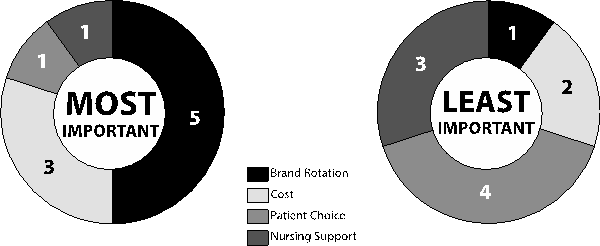
Figure 2: Factors listed as the most important and least important in determining the brand of growth hormone prescribed.
Growth Hormone Therapy
The numbers of patients treated with GH varied amongst respondents due to the variation in size of the centres: 0-9 (n=2, 20%), 10-25 (n=1, 10%), 16-49 (n=2, 20%), 50-99 (n=3, 30%), 100-150 (n=1, 10%), >150 (n=1, 10%). In deciding the GH preparation used, the most important factor was fair rotation between all brands (n=5, 50%), and the least important factor reported as patient choice (n=4, 40%) (Figure 2). Half of respondents had a general idea regarding the relative cost of each preparation of GH. All respondents would support the development of guidelines for GH prescribing in Ireland. Criteria considered necessary to be included in the guidelines include patient selection criteria (n=7, 70%), dose adjustment and discontinuation of therapy in failed response (n=8, 80%), restrictions on who should prescribe GH (n=8, 80%) and limitation to least costly products (n=5, 50%). Retaining the ability of trained endocrinologists to use clinical judgment in grey areas, or to have a committee for such cases was also recommended.
Growth Hormone Discontinuation
All respondents used height velocity (2-3 cm/yr) to guide discontinuation of therapy, while 4 (40%) also use bone age > 16 years as a guide. Three (30%) retest all patients following completion of therapy, while the remainder (n=7, 70%) stop therapy and review quality of life.
Discussion
We have described, for the first time, variations in the practice of diagnosis and treatment of GHD in Ireland. We have demonstrated variation at each stage of the diagnostic process, including measurement of infants and children, GHST (including sex steroid priming), diagnostic criteria used for GHD and criteria for discontinuation of treatment. We have also shown variation in selection of the particular GH prescribed. The recommendation for measuring children less than 2 years is for two people to measure the child using equipment with a moveable footplate18. Children over 2 years of age should be measured using a fixed stadiometer, without shoes. Standardisation of growth monitoring in paediatric practice in Ireland is required to ensure that faltering growth is accurately detected and, conversely, that measurement error does not misdiagnose healthy children with faltering growth. With recommendations under the new general practitioner contract for children under 6 years of age to incorporate regular measurement of children, it is important that facilities and training for accurate measurement are in place. The development of a standardised approach to GH treatment, and appropriate discontinuation where there is limited response to treatment, may also reduce the exposure of children to potential adverse effects. Recent studies have highlighted potential associations between childhood GH treatment and later morbidity such as bone tumors19 or early adult stroke20. While the methodology and conclusions of these studies have been disputed21, and not been replicated elsewhere22, this highlights the need for GH treated children to be enrolled in prospective international registries.
There are also economic implications of GH therapy for the healthcare system. Various brands and formulations of GH can cost over 50% more than others, despite comparable efficacy. Many prescribers are unaware of these cost differences and half of respondents rotate prescriptions between available brands rather than evaluate potential cost differences. This represents a potential area for future healthcare savings. Prescribing practices in Europe and Australia differ greatly from those in North America, due to differences in the license for GH, (i.e. prescribing regulation, indications, and doses used), and funding of this expensive treatment. There are strict criteria regulating the prescription of GH in Australia, through a program administered by the Department of Health with the assistance by an advisory committee, which comprises a panel of experienced paediatric endocrinologists23. In the UK the National Institute for Clinical Excellence24 specifically advocates use of the least costly GH product and specifies treatment criteria. We acknowledge the limitations of this study, specifically the low response rate amongst paediatricians. However there was an excellent response rate amongst paediatric endocrinologists. Nine respondents had completed subspecialty training in paediatric endocrinology, representing 90% of subspecialty trained paediatric endocrinologists practicing in Ireland at the time of the questionnaire. It is not possible to determine the standard of auxological measurement across paediatric clinics, but it is clear that this is sub-optimal in many centres both in terms of equipment and staffing. Furthermore, it is conceivable that height measurement in the community may be even less accurate than that provided in dedicated paediatric clinics due to lack of appropriate equipment and/or staff training in auxological techniques.
In summary, we have highlighted significant variation in practice related to childhood measurement and GH prescribing in Ireland. There is a need for the development of national guidelines in the evaluation and treatment of children with possible GHD, with a focus on cost effective, equitable and standardised care. We also recommend that a national registry be established for the longitudinal follow up of these patients. Accurate measurement of children is the cornerstone of growth assessment and we advise those providing care in clinics where children are measured, to ensure that auxological techniques and equipment are in accordance with national guidelines18.
Correspondence: SM O’Connell
Department of Paediatrics and Child Health, Cork University Hospital, Wilton, Cork
Email: [email protected]
Funding
CP Hawkes is supported by a PhD grant by the National Children’s Research Centre, Dublin.
References
- Rogol AD, Hayden GF. Etiologies and early diagnosis of short stature and growth failure in children and adolescents. J Pediatr. 2014 May;164:S1-14 e6.
- Job JC. Early diagnosis and early treatment of growth hormone deficiency. Horm Res.1989;31:149-52.
- Silvers JB, Marinova D, Mercer MB, Connors A, Cuttler L. A national study of physician recommendations to initiate and discontinue growth hormone for short stature. Pediatrics. 2010 Sep;126:468-76.
- Juul A, Bernasconi S, Clayton PE, Kiess W, DeMuinck-Keizer Schrama S, Drugs, Therapeutics Committee of the European Society for Paediatric E. European audit of current practice in diagnosis and treatment of childhood growth hormone deficiency. Horm Res. 2002;58:233-41.
- Lamp lM, Birch L, Picciano MF, Johnson ML, Frongillo EA, Jr. Child factor in measurement dependability. American journal of human biology: the official journal of the Human Biology Council. 2001 Jul-Aug;13:548-57.
- Himes JH. Minimum time intervals for serial measurements of growth in recumbent length or stature of individual children. Acta Paediatr. 1999 Feb;88:120-5.
- Lipman TH, Hench KD, Benyi T, Delaune J, Gilluly KA, Johnson L, Johnson MG, McKnight-Menci H, Shorkey D, Shults J, Waite FL, Weber C. A multicentre randomised controlled trial of an intervention to improve the accuracy of linear growth measurement. Arch Dis Child. 2004 Apr;89:342-6.
- Wilson TA, Rose SR, Cohen P, Rogol AD, Backeljauw P, Brown R, Hardin DS, Kemp SF, Lawson M, Radovick S, Rosenthal SM, Silverman L, Speiser P, Lawson Wilkins. Pediatric Endocrinology Society D, Therapeutics C. Update of guidelines for the use of growth hormone in children: the Lawson Wilkins Pediatric Endocrinology Society Drug and Therapeutics Committee. J Pediatr. 2003 Oct;143:415-21.
- Ghigo E, Bellone J, Aimaretti G, Bellone S, Loche S, Cappa M, Bartolotta E, Dammacco F, Camanni F. Reliability of provocative tests to assess growth hormone secretory status. Study in 472 normally growing children. J Clin Endocrinol Metab. 1996 Sep;81:3323-7.
- Gandrud LM, Wilson DM. Is growth hormone stimulation testing in children still appropriate? Growth Horm IGF Res. 2004 Jun;14:185-94.
- Tanaka T, Tachibana K, Shimatsu A, Katsumata N, Tsushima T, Hizuka N, Fujieda K, Yokoya S, Irie M. A nationwide attempt to standardize growth hormone assays. Horm Res. 2005;64 Suppl 2:6-11.
- Levy RA, Connelly K. Diagnostic growth hormone deficiency testing practices among patients in the NCGS/NCSS databases. J Pediatr Endocrinol Metab. 2003 May;16Suppl 3:619-24.
- MolinaS, Paoli M, Camacho N, Arata-Bellabarba G, Lanes R. Is testosterone and estrogen priming prior to clonidine useful in the evaluation of the growth hormone status of short peripubertal children? J Pediatr Endocrinol Metab. 2008Mar;21:257-66.
- Allen DB. Growth hormone post-marketing surveillance: safety, sales, and the unfinished task ahead. J Clin Endocrinol Metab. 2010 Jan;95:52-5.
- Cook DM, Yuen KC, Biller BM, Kemp SF, Vance ML, American Association of Clinical E. American Association of Clinical Endocrinologists medical guidelines for clinical practice for growth hormone use in growth hormone-deficient adults and transition patients – 2009 update: executive summary of recommendations. Endocrine practice : official journal of the American College of Endocrinology and the American Association of Clinical Endocrinologists. 2009Sep-Oct;15:580-6.
- Molitch ME, Clemmons DR, Malozowski S, Merriam GR, Vance ML, Endocrine S. Evaluation and treatment of adult growth hormone deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011 Jun;96:1587-609.
- vanHuis M, Bonthuis M, Sahpazova E, Mencarelli F, Spasojevic B, Reusz G,Caldas-Afonso A, Bjerre A, Baiko S, Vondrak K, Molchanova EA, Kolvek G, Zaikova N, Bohm M, Ariceta G, Jager KJ, Schaefer F, van Stralen KJ, Groothoff JW. Considerable variations in growth hormone policy and prescription in paediatric end-stage renal disease across European countries-a report from the ESPN/ERA-EDTA registry. Nephrology, dialysis, transplantation: official publication of the European Dialysis and Transplant Association – European Renal Association. 2015 Apr 28.
- Health Service Executive. Unit 6: Growth Monitoring 2012 [cited 2015].
- Carel JC, Ecosse E, Landier F, Meguellati-Hakkas D, Kaguelidou F, Rey G, Coste J. Long-term mortality after recombinant growth hormone treatment for isolated growth hormone deficiency or childhood short stature: preliminary report of the French SAGhE study. J Clin Endocrinol Metab. 2012 Feb;97:416-25.
- PoidvinA, Touze E, Ecosse E, Landier F, Bejot Y, Giroud M, Rothwell PM, Carel JC, Coste J. Growth hormone treatment for childhood short stature and risk of stroke in early adulthood. Neurology. 2014 Aug 26;83:780-6.
- Geffner ME, Santen R, Kopchick J. Growth hormone treatment for childhood short stature and risk of stroke in early adulthood. Neurology. 2015 Mar 10;84:1062-3.
- Savendah lL, Maes M, Albertsson-Wikland K, Borgstrom B, Carel JC, Henrard S, Speybroeck N, Thomas M, Zandwijken G, Hokken-Koelega A. Long-term mortality and causes of death in isolated GHD, ISS, and SGA patients treated with recombinant growth hormone during childhood in Belgium, The Netherlands, and Sweden: preliminary report of 3 countries participating in the EU SAGhE study. J Clin Endocrinol Metab. 2012 Feb;97:E213-7.
- Australian Government: The Department of Health. Pharmaceutical Benefits Scheme (PBS) Growth Hormone Program 2014 [cited 2015]. Available from: http://www.health.gov.au/internet/main/publishing.nsf/Content/health-pbs-general-supply-hghapplication.
- National Institute for Health and Care Excellence. Human growth hormone (somatropin) for the treatment of growth failure in children 2010 [cited 2015]. Available from: https://http://www.nice.org.uk/guidance/ta188.
Page 356