Introduction
It is a fallacy to believe that all clinical encounters between doctors and patients are amenable to satisfactory resolution and consequently uncertainty is a fact of life. Experienced doctors may modify this uncertainty through investigations. However, for newly qualified doctors this dilemma is compounded by both their limited knowledge and clinical experience1. In the Irish health care system, the most inexperienced doctor is often the first person to see and evaluate patients in the hospital setting adding to the clinical challenges that they encounter. This study was performed to evaluate clinical uncertainty, experienced in a hospital setting, from basic specialist paediatric trainee’s perspective.
Methods
Basic Specialist Trainees (BSTs) in paediatrics were surveyed while attending a study day. A 75% attendance rate of study days is required from the 64 BST in Paediatrics. The survey explored four aspects relating to uncertainty which included a) factors in decision-making, b) personal impact of uncertainty c) their response to clinical scenarios involving clinical error and challenges to their clinical decisions and d) potential strategies to address uncertainty. Data obtained included gender and year of graduation. A Likert scoring system was utilised (cuing at 1, not at all and at 6, definitely) to rate responses. A don’t know option was allowed to avoid coerced responses from trainees. Three trainee scenarios were assessed a) the response of trainees to a colleague who had made clinical error b) their response when a confident clinical decision was challenged by others and c) their response when the majority opinion differs from them in a clinical assessment. The survey was restricted to graduates with less than two years of clinical experience post internship to ensure a homogeneous group and to allow for generalisability of the results. This study received ethical approval from Mayo General Hospital research and ethics committee.
Results
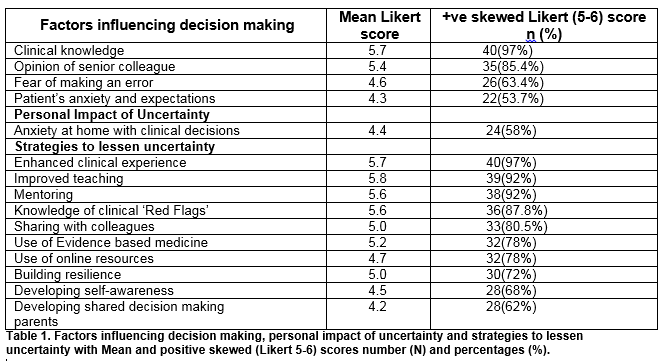
Forty-three (100%) trainees responded however only 41(93%) responses were incorporated into the analysis. Two trainees were excluded as they had more than three years’ paediatric experience. The Male: Female ratio was 1 to 2.9. Table 1 outlines factors influencing decision-making, the personal impact of uncertainty and the appropriateness of resources to address the uncertainty experienced by trainees. The mean Likert score with number and percentage of positive skewed response (Likert 5-6) for the clinical error scenario by a colleague were as follows: anger 1.4 and 0 (0%), anxiety 2.7 and four (9.4%), sympathy, 4 and 13 (32%), disappointment 2.1 and two (5%) and acceptance 3.7 and 21 (52.5%). The mean Likert score with number and percentage of positive skewed responses (Likert 5-6) for ‘having made a confident clinical decision scenario’ were as follows: likely to be swayed by a senior colleagues opinion 4.0 and 14 (34%) ,and likely to be swayed by patient 2.8 and three (8%).The response to the scenario where the majority opinion differs from the trainee were as follows :consider the alternate opinion and change one’s mind 32 (78%),try to convince others of your opinion 5 (12%), automatically concede three (7%),and adhere to one’s own opinion one (2.5%)
Discussion
This study was undertaken to evaluate junior doctors’ view on clinical uncertainty which is a combination of informational and intrinsic components. We are unaware of any similar study of Irish medical trainees. The factors that impact on clinical decision-making as indicated by positive skewed scores (Likert 5–6) were clinical knowledge in 38 (93%), the opinion of senior colleagues 35 85%), fear of making a mistake 26 (63%) and parental anxieties and expectations in 26 (54%). Trainees are influenced by senior colleagues as 32 (78%) would change their mind if challenged and 14(34%) will be swayed having made a confident clinical decision. Trainees experience significant distress with 24 (59%) reflecting frequently on patients encounters at home. Thirty-two percent of trainees are very sympathetic to colleagues who make errors and 53% accept that errors will occur. We did not assess if there were differences between male and female trainees.
Highly valued strategies (Likert score 5-6) to counteract information uncertainty included enhancing their clinical experience (97%), improved clinical teaching (95%), mentoring and support (93%), access to online clinical resources (78%), and enhanced evidence-based medicine teaching (78%). To address intrinsic uncertainty following strategies were highly favoured (Likert score 5-6) sharing uncertainty with colleagues (80%), building resilience (73%), developing self-awareness (68%) and integrating both parents and patients into shared care decisions (58%).
The traditional approach to junior doctor training is through experiential learning2. Senior colleagues inclusive of registrars, specialist register and consultants support this process through case-based discussion which is dependent on both clarity and accuracy of communication from the trainee and the understanding gleamed by the supervising colleague. In the early phase of training, the patient should be assessed by both the trainee and supervising doctor. Should this process not occur, the junior trainee is effectively obtaining a curbside consultation. Evidence suggests that this process is flawed, with a recent randomised controlled trial suggesting that in 51% of cases, the information was either inaccurate or incomplete or both which then translates into inappropriate management strategies3. If evidence is cited when offering advice to colleagues, the accuracy increases from 35% to 83%4, reinforcing the importance of substantiating one’s opinions with evidence.
Traditional medical education, with its focus on a good history and clinical examination leading to a diagnosis, does not facilitate the recognition of uncertainty that the trainee experiences. This difficulty is obviated if strategies are used that incorporate acknowledgement of the uncertainty experience e.g. utilising SNAPPS process for communication which has been shown to be effective in both ambulatory and acute care settings5 The mnemonic called SNAPPS consists of six steps: (1) Summarise briefly the history and findings; (2) Narrow the differential to 2 or 3 relevant possibilities; (3) Analyse the differential by comparing contrasting possibilities; (4) Probe the preceptor by asking questions about uncertainties, difficulties, or alternative approaches; (5) Plan management for the patient’s medical issues; and (6) Select a case-related issue for self-directed learning. This process is a learner centred technique that depends on the trainee for successful implementation and facilitates the expression of the diagnostic reasoning and recognising clinical uncertainties which the trainee may face6. Utilising this process takes less time that standard history. It modifies the teaching process where the supervising doctor role is changed from expert to facilitator7.
While utilising Evidence Based Medicine (EBM) to address clinical uncertainty appears intuitive, and is cited as an important strategy by trainees, it is not widely practiced. Currently the undergraduate medical curriculum in the US, Canada8 and Britain9 has an absence of formal assessment of EBM, with few medical schools incorporating the practice of evaluating EBM skills in their clinical assessments of students. A recent systematic review indicates that there is little published evidence demonstrating a transfer of evidence-based medicine into clinical practice10. This issue can only be addressed through the development and incorporation of evidence-based skills and practice into a national undergraduate medical curriculum which can move seamlessly into postgraduate education.
Intrinsic uncertainty is an inherent part of medical practice. However, trainees may have personality traits that predispose them to enhanced levels of uncertainty which can compromise medical care that they provide and increase the degree of stress that they experience. These uncertainty traits can be explored utilising the physician response to uncertainty scale which contains 15 items that evaluate: a) anxiety from uncertainty; b) concerns about bad outcomes; c) the reluctance to disclose uncertainty to patients; and d) evaluates the reluctance to this disclose mistakes to other doctors. This scale is useful in defining the presence of uncertainty in trainees 11and monitoring progress when appropriate interventions are put in place.
Uncertainty can be modified through the enhancement of trainee resilience12. Resilient doctors have low levels of emotional exhaustion and feelings of depersonalisation with a high rate of personal accomplishment. Trainee resilience is enhanced when a doctor enjoys his or her work, undertakes personal reflection, has a recognition of the limitations that medicine can achieve and has an ability to demarcate work from home life13. These skills must be both taught and practiced early in a doctor’s career to facilitate wellbeing and lessen uncertainty levels. While uncertainty is both informational and intrinsic, it can be modified through the appropriate teaching of knowledge related skills, inclusive of EBM strategies and the development of enhanced personal care skills, which should be incorporated into the training process, thus reducing the current distress that is being experienced by trainees in the medical profession giving credence to the maxim an ounce of prevention is work a pound of cure.
Competing Interest
None
Correspondence:
Dr Michael O’Neill,Dept of Paediatric Mayo University Hospital, Castlebar, Co.Mayo
Phone Number 087 8046896
Email: [email protected]
References
1 Han PK, Klein WM, Arora NK. Varieties of uncertainty in healthcare: a conceptual taxonomy.Med Decis Making.2011;31(6):828-838.
2 Bowen JL Educational strategies to Promote Clinical Diagnostic Reasoning.N Eng J Med 2006;355:2217-2225
3 Burden M, Sarcone E, Keniston A, Statland B, Taub JA, Allyn RL,Reid MB,Cervantes l,Frank MG,Scaletta n, Fung P,Chadaga SR,Mastalerz K,MallerN,Mascolo M,Zoucha J,Campbell J, Maher MP, Stella SA,Albert RK.Prospective Comparison of curbside Versus formal consultations. Journal of Hospital Medicine 2013; 8:31-35
4 Schaafsma F, Verbeek J, Hushof C, van Dijk F. Caution required when relying on colleagues advice; a comparison between professional advice and evidence from the literature Health Serv Res 2005 Aug31:5:59
5 Wolpaw TM, Wolpaw DR, Pappp KK. SNAPPS :A learner Model for Outpatient Education.Acad Med 2003;78:893-898
6 Wolpaw T, Cote L, Papp KK, Bordage G.Student uncertainties drive teaching during Case Presentations:More so with SNAPPS. Academic Medicine 2012;87:1210-1217
7 E Pascoe JM, Nixon J, Lang VJ.Maximising Teaching on the Wards: Review and Applications of the One-Minute Preceptor and SNAPPS model.Journal of Hospital Medicine 2015;10:125-130
8 Blanco MA, Capello CF, Dorsch JL, Perry G, Zanietti ML.A Survey of Evidence -Based Medicine Training in the US and Canadian Medical Schools.J Med Lib Assoc 2014;102:160-168
9 Meats E, Heneghan C, Crilly M, Glasziou Evidence Based Medicine Teaching in UK Medical Schools.Medical Teacher 2009;31:369-374
10 Ahmadi SF, Baradaran HR, Ahmadi E. Effectiveness of teaching Evidence Based Medicine to undergraduate medical Students:A BEME systematic Review. Medical Teacher 2015;37:21-30
11 Politi MC, Clark MA, Ombao H, Legare F, The Impact of Physicians Reactions to Uncertainty on Patients’Decision Satisfaction. J Eval Clin Pract 2011;17:575-578
12 Leppin AL, Bora PR,Tilburt JC, Gionfrido mR, Zeballos-Palacios C, Dulohery NM, Sood A ,Erwin PJ,Brito JP, Boehmer KR, Montori VM.The Efficacy of Resiliency Training programs: A Systematic Review and Meta Analysis of Randomised Trials. PloS One. 2014;9(10):e111420
13 Zwack J, SchweitzerJ. If every fifth Pyysician is affected by Burnout, what about the other four.Resilience Strategies of Experienced Physicians.Acad Med 2013;88:382-388
p581