Introduction
Schwartz rounds (SR) are a multi-disciplinary intervention that aim to support clinical and non-clinical healthcare professionals in their work. Temple Street Children’s University Hospital (TSCUH) is the first paediatric hospital to introduce SR. SR are a popular intervention, with numerous sites adopting them in the US and the UK. 1 First introduced in Ireland in 2015, they were piloted at sites in Galway University Hospital and Blackrock Hospice. 2 SR have since spread to 15 other sites across Ireland, including regional hospitals, children’s hospices and ambulance services. 2 Only one paper has been published on the topic of SR in paediatric hospitals.3 This paper hopes to highlight the potential for SR in the paediatric context by evaluating the views of staff who attended SR at TSCUH.
SR are hour long meetings where a panel of three or four staff share their personal stories surrounding a preselected theme. The themes may be general, such as ‘A Challenging Patient’ or specific, such as ‘The Magic of Temple Street’. After the panellists present their stories, the floor is open to discussion, which is moderated by a trained facilitator. Participants may reflect on the stories shared and share their own. The Point of Care Foundation (POCF) offers detailed guidelines on how SR should be run and provide a two-day training course for the facilitators.4 This involves face to face workshops and require some previous exposure to SR prior to training. Institutional support was sought and subsequently the team involved in this research undertook training and receive ongoing supervision from the POCF.4 In Ireland, HSE funding supports training.
SR were developed with the aim of supporting caregivers in providing compassionate care for their patients. 5 One potential barrier to this is burnout- extant literature widely documents both the rates and consequences of burnout in healthcare professionals. 6 Several recent editorials highlight this topic. 7 Serious negative effects on important metrics like patient safety and staff morale are demonstrated. 8 Irish clinicians are reporting significant difficulties in relation to burnout. 9 Hayes et al explored burnout in Ireland by surveying junior doctors in the Wellbeing of Hospital Doctors in Ireland report.10 Hayes et al found that one third of Irish doctors are suffering from burnout. Many participants mentioned wanting to leave the healthcare profession altogether. Thus it is of great importance that the Irish health system takes a proactive approach to the issue. SR are an evidenced intervention supporting teamwork and compassionate care. One protective factor against burnout appears to be teamwork.11 Clinicians who perceive that teamwork is good in their work environment have lower rates of burnout compared to their colleagues.12 SR can improve appreciation of colleagues across disciplines. 13 As having a strong sense of teamwork has been found to be protective against burnout, SR may help prevent other negative consequences of burnout, like poor patient safety14.
Methods
This is an opt-in study of hospital staff who attended SR and completed a feedback form. Ethics approval was sought and granted. The data for this paper was collected from the standard feedback forms that participants filled immediately after the round. It was not possible to identify repeat attendees (forms were submitted anonymously). Likert scales were rated from 1-5, with 5 as the most positive. Responses were transcribed into an Excel worksheet, which was then transferred into SPSS for quantitative analysis. The qualitative analysis of the comment section was done via thematic analysis, as outlined by Braun and Clarke.15
Results
The total number of feedback forms returned was 198 over five rounds. The themes of the five rounds were: ‘A Patient I’ll Never Forget’, ‘The Magic of Temple Street Hospital’, ’Brief Encounters’, ‘Challenging Patients’, and ‘Snow Days’. The average response rate was 67%. The average amount of days between rounds was 42, with the highest being 62 and the lowest being 23 days. The overall attendance for the rounds was 295, with a high of 93 and a low of 25. The average attendance at each round was 59. Better attendance was evident when rounds were held at lunchtimes.
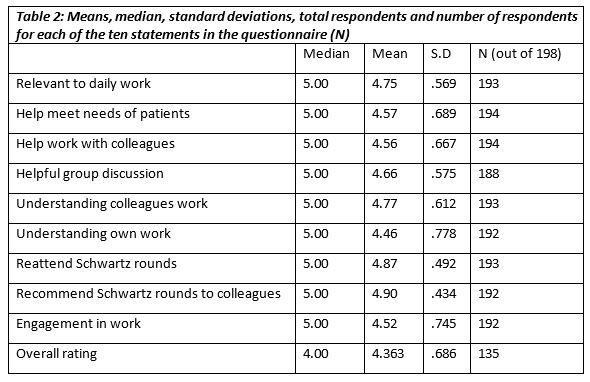
In 95% (n=189) of the returned forms, the statements were all rated positively. Not all forms were fully completed (some questions left blank) but all were included in the analysis. The statements were shown to be highly correlated with each other (Cronbach’s alpha = 0.89). The statement associated with the highest amount of agreement was ‘I would recommend Schwartz Centre Rounds to colleagues’, with 90% (n=178) selecting ‘Completely agree’. The statement associated with the lowest amount of agreement was ‘I have a better understanding of how I feel about my work’, with 58% (n=116) selecting completely agree. The rating of the rounds also reflected the positive response, with 62% (n=124) of respondents rating the round as excellent or exceptional.

Based on the median response to the eight statements on the feedback form, there was a high degree of agreement between the professions. In terms of clinical versus non-clinical staff attendance, 65.2% (n=129) were clinical while 29.8 % (n=59) were non-clinical. A Kruskal-Wallis test (p= .466) showed there was no significant difference between clinical and non-clinical staff in terms of their median overall response to the statements about the rounds. A chi squared test (c2 (4) = 8, p = .074), also showed this.
Overall there were 84 comments from the five rounds, giving an overall response rate of 42%. There were three apparent main themes, which are outlined in Table 3. The As there was a limited number of comments, it was not meaningful to break down some of the themes into smaller categories.
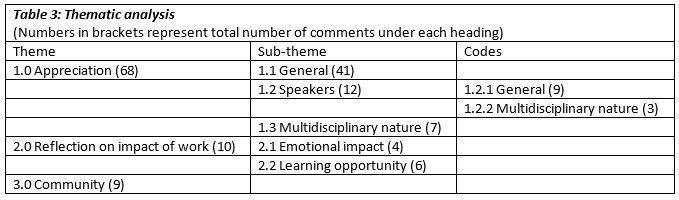
The general appreciation comments were typically participants congratulating the facilitators on a job well done or thanking them for running the round. There was no pattern in terms of difference in opinion between profession revealed in the comments. For the comments on the speakers, they either fell into the area of praise or were a comment on multidisciplinary nature of the speakers:
“Excellent speakers, stories. Really admire speakers' honesty. Thank you for sharing; you are brilliant!"
"Thank you to all the presenters for their bravery in telling their stories. Thank you for sharing:)"
"Very engaging stories from variety of disciplines. Very thought provoking.”
This theme of appreciating the multidisciplinary nature of SR showed up in a more general way in the comments:
“Exceptional, very moving, great to hear the multidisciplinary view of their experiences.”
The comments on reflection fell into one of two themes, emotional impact and learning opportunities:
“An excellent session, very moving and thought provoking. Great to have a space to reflect on the emotional impact of our work. Thank you.”
“Fantastic forum to reflect and consider challenges. Good MDT input and greater understanding of challenges across all clinical area.”
The comments on community were typically about how SR is a good forum for reinforcing or building a sense of staff community:
“Ah lads! Just lovely. Reinforcing our wonderful sense of community.”
Discussion
This paper is an evaluation of a pilot program of SR run in TSCUH over a period of seven months, from September 2017 to March 2018. Both quantitative and qualitative analysis were performed. The purpose of this evaluation is to determine the views of the staff of TSCUH on SR. This is also the first pilot of these rounds in a paediatric hospital in Ireland.
This pilot has been positively received by a range of disciplines, both clinical and non-clinical. This reflects the findings of other evaluations of SR.14 The commentary revealed that there was a varied perception in terms of SR utility in TSCUH, with some staff focusing on how SR would help them relate to their patients and others their colleagues .Literature published on the topic of SR in the UK that shows that the model has transitioned well from US to UK culture. 11, 16 Based on the high adoption rate and the results of this evaluation, this intervention appears a feasible and acceptable approach in a paediatric hospital in Ireland.
In practical terms, implementation in busy hospital environments comes with challenges. The pattern that the best attended rounds were held at lunch times was a helpful finding for future SR in TSCUH. Due to the nature of hospital staff work, it can be very difficult to accommodate attendance of all staff groups at every single round. For instance, while the lunch rounds were the best attended, nurses mostly attended rounds held in the morning due to the structure of their shifts. This pilot also provides practical information regarding feedback. Around 30% (n=63) of respondents did not complete an overall rating for the rounds on the form. Future delivery will consider these results to ensure we meet the needs of the attendees, including modification of feedback forms and allowing flexibility of SR timing so that a diversity of staff groups can attend, and to embed this intervention into hospital culture in a responsive, flexible and inclusive way.
There were some limitations in this evaluation. The feedback forms are filled out immediately after the round. While this does have some benefits in terms of avoiding recall bias, it may limit the scope of what can be deduced. For example, it is not possible to evaluate any long-term impact that SR may have on practice with this method. One possible valuable approach would be a comparison of TSCUH with another Irish paediatric hospital that does not run SR. Ideally this would take the form of a longitudinal study, in order to provide a meaningful measure of impact. A qualitative study of regular SR attendees (compared with non-attendees) within TSCUH would be informative. It is important that interventions such as SR are evaluated, so that they are utilised for maximum benefit to attendees and indeed the institution. We are cognizant that in a resource depleted health system, expenditure must be carefully considered. In the United States, SR have been shown to have a positive influence on hospital culture, helping to create a working environment to support compassionate care. 17 A recent Cochrane review also concluded that interventions such as SR did appear to have benefit for staff. 18
Finally, we do not propose that Schwartz rounds are a sole solution for the many barriers to compassionate care that hospital staff face, but we identify that it is critical that institutional support across hospitals be developed. A major cause of burnout that has been identified is the working conditions that clinicians face. 19,20 Hayes et al recommended that organisations should focus on the welfare of staff in making their polices .10 West et al propose other interventions such as mentoring and Shanafeld et al have highlighted other institutional approaches. 21 , 7 SR are an example of how organisations can try to improve working conditions of staff by giving them a space where they feel listened to. The Kings Fund report showed that participants saw SR as a way to strengthen team bonds within the hospital. 22 A follow up report on SR in the UK found that there was a correlation between attendance at SR and psychological well-being, as measured by a reduction in GHQ-12 scores.11 This is worth exploring in the longer term in Ireland. Schwartz rounds are a well evidenced and well received intervention that support clinician engagement, foster compassion and interdisciplinary working.
Acknowledgments
We wish to thank all participants on the Schwartz Rounds panels, colleagues from across the hospital who attended and shared their experiences and views, and the hospital HR and CEO who supported this initiative.
Conflicts of Interest Statement
None of the authors have a conflict of interest to be declared.
Corresponding Author
Dr. Elizabeth Barrett
Temple Street Children’s University Hospital,
Temple Street,
Dublin 1
Email: [email protected]
References
1. The Schwartz Centre. Schwartz Center Healthcare Members | The Schwartz Center for Compassionate Healthcare [Internet]. 2018 [cited 2018 Jul 4]. Available from: http://www.theschwartzcenter.org/join-us/become-healthcare-member/schwartz-center-members/
2. The Point of Care Foundation. Locations | Point of Care Foundation [Internet]. 2018 [cited 2018 Jul 4]. Available from: https://www.pointofcarefoundation.org.uk/locations/
3. Hughes J, Duff AJ, Puntis JWL. Using Schwartz Center Rounds to promote compassionate care in a children’s hospital. Arch Dis Child. 2018;103(1):11–2.
4. Facilitator and clinical lead training | Point of Care Foundation [Internet]. [cited 2019 Apr 6]. Available from: https://www.pointofcarefoundation.org.uk/our-work/schwartz-rounds/training/
5. Robert G, Philippou J, Leamy M, Reynolds E, Ross S, Bennett L, Taylor C, Shuldham C, Maben J, Philippou RG, Leamy J. Exploring the adoption of Schwartz Center Rounds as an organisational innovation to improve staff well-being in England. BMJ Open [Internet]. 2009 [cited 2018 Jun 10];7. Available from: http://dx.doi.org/10.1136/
6. Lemaire JB, Wallace JE. Burnout among doctors. BMJ [Internet]. 2017 Jul 14 [cited 2018 May 30];358:j3360. Available from: http://www.ncbi.nlm.nih.gov/pubmed/28710272
7. Shanafelt TD, Lee T, Gunderman R, Strongwater S, Sinsky C. Physician Burnout: The Root of the Problem and the Path to Solutions. NEJM Catalyst. Waltham, MA: NEJM Catalyst; 2017.
8. Epstein RM, Privitera MR. Doing something about physician burnout. Lancet [Internet]. 2016 Nov [cited 2018 Jun 27];388(10057):2216–7. Available from: https://ac-els-cdn-com.ucd.idm.oclc.org/S0140673616313320/1-s2.0-S0140673616313320-main.pdf?_tid=35b9ae3a-7ff9-4853-a04f-4c0cf2059735&acdnat=1530091341_fe8b424153966a2ecb3c455726e12bb7
9. O’Connor P, Lydon S, O’Dea A, Hehir L, Offiah G, Vellinga A, Byrne D. A longitudinal and multicentre study of burnout and error in Irish junior doctors. Postgrad Med J [Internet]. 2017 Nov 1 [cited 2018 Jun 5];93(1105):660–4. Available from: http://www.ncbi.nlm.nih.gov/pubmed/28600343
10. Hayes B, Walsh G, Prihodova L. NATIONAL STUDY OF WELLBEING OF HOSPITAL DOCTORS IN IRELAND [Internet]. 2017 [cited 2018 Jul 10]. Available from: www.rcpi.ie/physician-wellbeing
11. Maben J, Taylor C, Dawson J, Leamy M, McCarthy I, Ross S, Shuldham C, Bennett L, Foot C. A realist informed mixed methods evaluation of Schwartz Center Rounds® in England: First look draft. 2017.
12. Welp A, Meier LL, Manser T. The interplay between teamwork, clinicians’ emotional exhaustion, and clinician-rated patient safety: a longitudinal study. Crit Care [Internet]. 2016 Dec 19 [cited 2019 Apr 6];20(1):110. Available from: http://www.ncbi.nlm.nih.gov/pubmed/27095501
13. Reed E, Cullen A, Gannon C, Knight A, Todd J. Use of Schwartz Centre Rounds in a UK hospice: Findings from a longitudinal evaluation. J Interprof Care [Internet]. 2015 Jul 4 [cited 2019 Apr 6];29(4):365–6. Available from: http://www.tandfonline.com/doi/full/10.3109/13561820.2014.983594
14. Goodrich J, Cornwell J. The contribution of Schwartz Center Rounds® to hospital culture. [cited 2018 Jul 10]; Available from: https://www.kingsfund.org.uk/sites/default/files/field/field_publication_file/contribution-schwartz-center-rounds-goodrich-cornwell-may12.pdf
15. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol [Internet]. 2006 Jan [cited 2018 Jun 27];3(2):77–101. Available from: http://www.tandfonline.com/action/journalInformation?journalCode=uqrp20
16. Chadwick RJ, Muncer SJ, Hannon BC, Goodrich J, Cornwell J. Support for compassionate care: Quantitative and qualitative evaluation of Schwartz Center Rounds in an acute general hospital. JRSM Open [Internet]. 2016 Jul [cited 2018 May 21];7(7):205427041664804. Available from: http://www.ncbi.nlm.nih.gov/pubmed/28050259
17. Lown BA, Manning CF. The Schwartz Center Rounds: Evaluation of an Interdisciplinary Approach to Enhancing Patient-Centered Communication, Teamwork, and Provider Support. Acad Med [Internet]. 2010 Jun [cited 2018 May 23];85(6):1073–81. Available from: https://insights.ovid.com/crossref?an=00001888-201006000-00037
18. Reeves S, Pelone F, Harrison R, Goldman J, Zwarenstein M. Interprofessional collaboration to improve professional practice and healthcare outcomes. Cochrane Database Syst Rev [Internet]. 2017 Jun 22; Available from: http://doi.wiley.com/10.1002/14651858.CD000072.pub3
19. O’Connor K, Muller Neff D, Pitman S. Burnout in mental health professionals: A systematic review and meta-analysis of prevalence and determinants. Eur Psychiatry [Internet]. 2018 Sep [cited 2018 Jul 10];53:74–99. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0924933818301275
20. Jovanović N, Podlesek A, Volpe U, Barrett E, Ferrari S, Rojnic Kuzman M, Wuyts P, Papp S, Nawka A, Vaida A, Moscoso A, Andlauer O, Tateno M, Lydall G, Wong V, Rujevic J, Platz Clausen N, Psaras R, Delic A, Losevich MA, Flegar S, Crépin P, Shmunk E, Kuvshinov I, Loibl-Weiß E, Beezhold J. Burnout syndrome among psychiatric trainees in 22 countries: Risk increased by long working hours, lack of supervision, and psychiatry not being first career choice. Eur Psychiatry [Internet]. 2016 Feb 1 [cited 2018 May 31];32:34–41. Available from: https://www.sciencedirect.com/science/article/pii/S0924933815006768
21. West CP, Dyrbye LN, Erwin PJ, Shanafelt TD. Interventions to prevent and reduce physician burnout: a systematic review and meta-analysis. Lancet [Internet]. 2016 Nov [cited 2018 May 30];388(10057):2272–81. Available from: https://ac-els-cdn-com.ucd.idm.oclc.org/S014067361631279X/1-s2.0-S014067361631279X-main.pdf?_tid=10c571d7-a0ae-41c6-8337-038cecdec3a0&acdnat=1527700707_c7a57bd74d4da32691b72d0d6b246427
22. Goodrich J. Schwartz Center Rounds Evaluation of the UK pilots: Are you seeing the person in the patient? [Internet]. 2011 [cited 2018 Jun 23]. Available from: www.kingsfund.org.uk
Issue: Ir Med J; Vol 112; No. 6; P951