D Lillis, C Lloyd, P O’Kelly, S Kelada, S Kelly, P Gilligan
Emergency Department, Beaumont Hospital, Dublin 9
Abstract
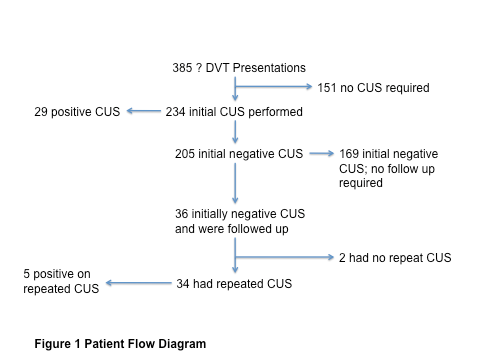
Pre-test probability scoring and blood tests for deep venous thrombosis (DVT) assessment are sensitive, but not specific leading to increased demands on radiology services. Three hundred and eighty-five patients presenting to an Emergency Department (ED), with suspected DVT, were studied to explore our actual work-up of patients with possible DVT relating to risk stratification, further investigation and follow up. Of the 205 patients with an initially negative scan, 36 (17.6%) were brought for review to the ED Consultant clinic. Thirty-four (16.6%) patients underwent repeat compression ultrasound with 5 (2.4%) demonstrating a DVT on the second scan. Repeat compression ultrasound scans were performed on 34 (16.6%) patients with an initially negative scan, with essentially the same diagnostic yield as other larger studies where 100% of such patients had repeat scanning. Where there is ongoing concern, repeat above-knee compression ultrasound within one week will pick up a small number of deep venous thromboses.
Introduction
Deep Venous Thrombosis (DVT) occurs in 84 people per 100,0001. The 9th Edition of the American College of Chest Physicians guidelines advocate the use of an objective method of risk stratification. Clinical assessment alone has proven unreliable2,3. Algorithms using a combination of a pre-test probability score, D-Dimer, and ultrasonography are now the norm. The most commonly used pre-test probability score is the Wells score, which combines patients’ symptoms, signs and history to provide a risk stratification for the possibility of DVT4. D-Dimer is a sensitive but not specific marker for DVT5. Elevated levels are also seen in the presence of infection, inflammation, malignancy, and trauma. Above-knee or whole-leg ultrasonography are now the imaging modalities of choice. In above-knee-only compression ultrasound, the inability to compress the femoral and popliteal veins under gentle pressure, visualisation of thrombus and lack of augmentation of flow on manual compression of the calf muscles are considered diagnostic of a DVT. Propagation into the proximal venous system of an isolated calf vein DVT generally occurs within 5 to 7 days6. In order to detect extension, repeat compression ultrasonography within one week should be performed according to some authors7,8. Whole-leg ultrasound has been advocated as a once off investigation for DVT9. It detects DVTs in both the proximal and distal venous system, obviating the need for repeat testing. However, debate is ongoing as to whether isolated distal DVTs are clinically relevant, and whether they require anticoagulation with its associated risks3. This study was conducted to assess the investigation of DVT over a one-year period in an adult ED in the context of performance of pre-test probability risk stratification, D-Dimer, and ultrasound investigation.
Methods
The study was conducted in the Emergency Department of a large teaching hospital providing care to 50,000 ED presentations per year. During the working week, patients presenting with a possible DVT were assessed by a Clinical Nurse Specialist (CNS) service within the department. This is overseen by the senior Emergency Clinician. Each patient was managed according to a DVT algorithm consisting of a pre-test probability score (Wells score), D-Dimer and if indicated, ultrasonography. Outside of these hours, the assessment was made by the ED medical team. Patients with a low pre-test probability as evidenced by the Wells score and who had a negative D-Dimer were discharged. Patients with a ‘DVT likely’ pre-test Wells score and a positive or negative D-Dimer had an initial above-knee ultrasound. If this was negative, a decision was made as to whether the patient was required to attend an ED review clinic and potentially have a repeat ultrasound. All ultrasonographic examinations were conducted in the radiology department by ultrasound radiographers. The images were subsequently interpreted by a radiologist. A retrospective study of all patients who presented to the Emergency Department with suspected Deep Venous Thrombosis (DVT) in the year 2010 was performed. Ethical approval for the study was granted by the Beaumont Hospital Research Ethics Committee.
Three sources of potential DVT patient details were searched: the DVT nurse specialist’s logbook, the six ultrasound logbooks for 2010 and the ED review clinic book for the year were used. Blood results, presenting complaints and the ultrasound results for patients were all retrieved using the Patient Information Profile Explorer system, an internal information technology system used in the hospital. All data from the computer system were cross-referenced with the information taken from the other three sources. Data for 404 patients was collected. Nineteen (4.7%) were excluded due to an incomplete data set. Logistic regression modelling was used for the statistical analysis with odds ratios (OR), and 95% confidence intervals (CI), used to define relative risk of a positive score. Univariate methods were initially employed, and subsequently multi-factorial models were implemented to determine independently significant variables in the presence of potential confounders. Box plots were used to describe D-Dimer and Wells scores between US groups. A P-value < 0.05 was deemed to be significant. Statistical analysis was conducted using Stata (version 10, College Station, Texas).
Results
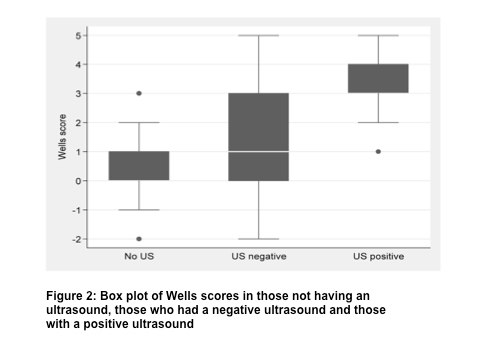
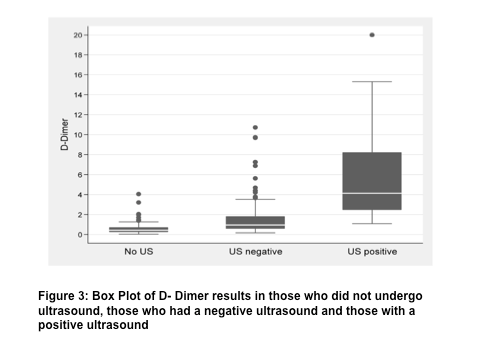
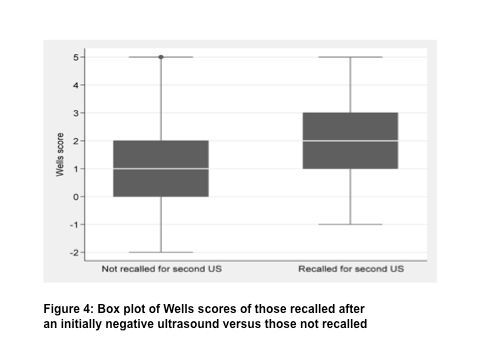
The flow of patients through the investigation algorithm is demonstrated in figure 1. Of the initial 385 patients, 151 (39.2%) had a low pre-test probability, negative D-Dimer, and did not require further investigation. Of the 234 patients who underwent ultrasound scan, 29 (12.4%) patients had a positive above knee compression ultrasound scan (CUS). Of the 205 with an initially negative scan 169 (82.4%) were deemed not to require a repeat ultrasound. Thirty-six (17.6%) patients whose initial scan was negative were sent to the ED review clinic, of whom 34 had repeated ultrasonography. Five (14.7%) of these patients had a positive scan. As expected, patients who had a positive result on compression ultrasonography were more likely to have a significantly higher mean pre-test probability (Wells) score. Those with a negative scan were more likely to have a higher score than those who received no scan at all. Logistic regression (multifactorial model) for a positive US result showed (Wells) score to be highly significant (OR 3.1, CI 1.76- 5.44, P<0.001). Higher D-Dimer results were found in those with a positive scan. Patients who were referred for an initial ultrasound had significantly higher mean D-Dimer results than those who did not have any imaging. Logistic regression for a positive US outcome demonstrated significance for high D-Dimer (OR 1.43, CI 1.16-1.75, P=0.001). Patients who attended the review clinic and had repeated ultrasonography, had a significantly higher mean pre-test probability score and again regression analysis of a positive outcome showed this to be significant (OR 1.55, CI 1.08- 2.22, P =0.015).
Discussion
The data from the 385 patients included in this study demonstrate significant correlation with previous research conducted by Wells et al.4,5,10 insofar as those patients diagnosed with a DVT were more likely to have a high pre-test probability score (P <0.001, OR 3.1, CI 1.76- 5.44). This confirms that in our department pre-test probability, informs the decision to investigate further. Clinicians were more likely to refer patients to the review clinic if they had higher pre-test probability scores with a view to a repeat ultrasound being performed, suggesting that, despite a negative initial scan, the clinician remained concerned about the possibility of a DVT. As expected, when the D-Dimer results were correlated between the ‘no ultrasound performed’, ‘negative ultrasound’ and ‘positive ultrasound’ groups, those patients with a DVT were more likely to have higher D-Dimer values (P<0.001, OR 1.4, CI 1.16-1.75). Those with a higher D-Dimer value after an initially negative compression ultrasound were more likely to be sent to the review clinic and have a repeat scan. Therefore, marked elevation of the D-Dimer was associated with ongoing clinical concern, even when initial scans were negative. The pre-test probability scores and D-Dimer values overlap between the patients not referred for a second scan and those who were. We would suggest that the pre-test score, D-Dimer, history and examination are not taken in isolation but combined to inform the clinical decision as to whether or not to perform a second ultrasound. This decision-making process resulted in only 36 (17.6%) of a possible 205 patients with initially negative scans being asked to attend the review clinic. Five (2.4% of those with an initially negative scan) of whom had a DVT on repeat scan.
With regard to repeated above knee only compression ultrasonography or once off whole leg scanning, the recent ACCP guidelines have advocated patient preference, such as those unable to return for serial testing, and institutional access as factors in the decision to utilise one modality over the other3. Bernardi et al. conducted a prospective, randomised, multicentre study of consecutive symptomatic outpatients (n=2098) with a first episode of suspected DVT of the lower extremities11. Patients were randomised to undergo 2-point compression ultrasound with D-Dimers, or whole-leg ultrasonography. The main outcome measure was a confirmed 3-month incidence of symptomatic venous thromboembolism in patients with an initially normal diagnostic workup. In the compression ultrasound/ D-Dimer group, the initial diagnostic yield was 20.7% (12.4% in our study). Of the 256 patients with a normal compression ultrasound but abnormal D-Dimer, 5.4% were found to have a proximal DVT on the repeated compression ultrasound (2.4% of patients in our study). Ten patients (26.4%) of the whole leg ultrasound group were diagnosed with an above or below-knee DVT and anti-coagulated. At three-month follow up, the study found that symptomatic venous thromboembolism occurred in 7 of 801 patients (0.9%) in the 2-point compression ultrasound group and in 9 of 763 patients (1.2%) in the whole-leg group. They concluded that the two strategies were equivalent. In this context, our department’s strategy of performing above-knee ultrasound would appear reasonable.
Rather than all patients with an initially negative scan undergoing repeat above knee compression ultrasound, in our study only 16.6% (34/205) of patients did. 14.7% (5/34) demonstrated a DVT on the repeat scan where the initial scan had been negative. Five out of 205 (2.4%) patients who had an initially negative compression ultrasound, demonstrated a DVT on repeat scan. This detection rate from a repeated scan is in line with other large-scale studies, which demonstrate a diagnostic yield of 2%12,13. One hundred and seventy one fewer repeat compression ultrasound scans were performed with a targeted approach of repeat above-knee ultrasound with the same diagnostic yield as in studies where all patients were re-scanned. The data would suggest that clinicians on the emergency department floor are using pre-test probability scores, D-Dimer results and clinical gestalt to influence their clinical assessment of the patients’ complaint and in deciding on whether or not to perform an initial and repeated compression ultrasound. In doing so, large savings can be made in terms of ultrasonography, staff labour, and the financial burden on patients having to re-attend the hospital. This study was performed in a single ED and so may not apply to other settings. Nineteen of the original 404 population had an incomplete data set and were not included in the study, which may have influenced the results. Kappa values evaluating inter-rater reliability regarding the calculation of Wells Scores were not calculated.
Decision making is what doctors do and whilst guidelines assist us, ultimately we make an informed decision in the best interests of our patients. This study demonstrates the same diagnostic yield for DVT on repeat scanning as other international studies but with significantly less repeat diagnostic testing. In the context of an initially negative above-knee compression ultrasound with a positive D-Dimer, where there is ongoing concern, a repeat ultrasound within one week will pick up a small number of deep venous thromboses.
Correspondence: P Gilligan
Emergency Department, Beaumont Hospital, Dublin 9
Email: [email protected]
References
- Anderson FA Jr, Wheeler HB, Goldberg RJ, Hosmer DW, Patwardhan NA, Jovanovic B, Forcier A, Dalen JE. A population based perspective of the hospital incidence and case-fatality rates of deep vein thrombosis and pulmonary embolism. The Worcester DVT Study Arch Intern Med 1991;151:933–8.
- Guyatt GH, Akl EA, Crowther M, Gutterman DD, Schunemann HJ. Executive Summary: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines Chest 2012;141:7S-47S
- Bates SM, Jaeschke R, Stevens SM, Goodacre S, Wells PS, Stevenson MD, Kearon C, Schunemann HJ, Crowther M, Pauker SG, Makdissi R, Guyatt GH; American College of Chest Physicans. Diagnosis of DVT: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines Chest. 2012; 141:e351S-e418S.
- Wells PS, Owen C, Doucette S, Fergusson D, Tran H. Does This Patient Have Deep Vein Thrombosis? JAMA 2006;295:199-207.
- Wells PS, Anderson DR, Bormanis J, Guy F, Mitchell M, Lewandowski B. SimpliRED D-Dimer can reduce the diagnostic tests in suspected deep vein thrombosis Lancet 1998;351:1405-6.
- Kearon C, Julian JA, Newman TE, Ginsberg JS. Noninvasive diagnosis of deep venous thrombosis. McMaster Diagnostic Imaging Practice Guidelines Initiative Ann Intern Med 1998;128:663-677
- Kearon C, Ginsberg JS, Douketis J, Crowther, MA, Turpie AG, Bates SM, Lee A, Brill- Edwards P, Finch T, Gent M. A Randomized Trial of Diagnostic Strategies after Normal Proximal Vein Ultrasonography for Suspected Deep Venous Thrombosis: D-Dimer Testing Compared with Repeated Ultrasonography Ann Intern Med 2005;142:490-496
- Dewar C, Selby C, Jamieson K, Rogers S. Emergency department nurse-based outpatient diagnosis of DVT using an evidence-based protocol Emerg Med J 2008;25:411–416
- Zierler BK. Ultrasonography and diagnosis of venous thromboembolism Circulation 2004; 109:I9-I14
- Wells PS, Anderson DR. Diagnosis of deep-vein thrombosis in the year 2000. Curr Opin Pulm Med 2000;6:309-313.
- Bernardi E, Camporese G, Büller HR, Siragusa S, Imberti D, Berchio A, Ghirarduzzi A, Verlato F, Anastasio R, Prati C, Picciolo A, Pesavento R, Bova C, Maltempi P, Zanatta N, Cogo A, Cappelli R, Bucherini E, Cuppini S, Noventa F, Prandoni P; Erasmus Study Group. Serial 2-Point Ultrasonography Plus D-Dimer vs Whole-Leg Color-Coded Doppler Ultrasonography for Diagnosing Suspected Symptomatic Deep Vein Thrombosis. A Randomized Controlled Trial JAMA 2008;300:1653- 1659
- Michiels JJ, Gadisseur A, Van Der Planken M, Schroyens W, De Maeseneer M, Hermsen JT, Trienekens PH, Hoogsteden H, Pattynama PM. A critical appraisal of non-invasive diagnosis and exclusion of deep vein thrombosis and pulmonary embolism in outpatients with suspected deep vein thrombosis or pulmonary embolism: how many tests do we need? Int Angiol 2005;24:27–39
- Cogo A, Lensing AW, Koopman MM, Piovella F, Sirgusa S, Wells PS, Villalta S, Buller HR, Turpie AGG, Prandoni P. Compression ultrasound for diagnostic management of patients with clinically suspected deep-vein thrombosis: prospective cohort study. BMJ 1998;316:17–20.