Introduction
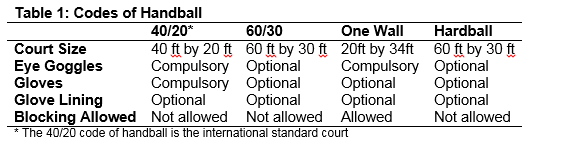
One of Ireland’s national sports is Gaelic handball (which should not be confused with Olympic handball). It is similar to squash except the ball is struck with the hand. Itis estimated that 13,000 Irish people play the game1. Gaelic handball involves two or four players (singles or doubles). Four different codes of Gaelic handball are played in both indoor and outdoor alleys. Table 1 indicates key characteristics that differentiate between the different codes of Gaelic handball. It is generally accepted that an epidemiological study is necessary in order to develop effective injury prevention mechanisms to reduce the rate of injury2. However to date there are no published studies on Gaelic handball. The aim of this study is to assess the epidemiology of injury in Gaelic handball. Information on the demographic profile of Gaelic handball players, training load, warm up activities and the protection equipment utilised will also be provided. For the remainder of the article handball will refer to Gaelic handball only.
Methods
Seventy five handball players (14-66 years) completed a self-report questionnaire that was based on a retrospective questionnaire implemented in Gaelic footballers3. The questionnaire comprised of 28 questions and was divided into two sections. Section one related to the participants’ body dimensions, type and amount of handball played, limb dominance, injury prevention methods used and other sports played. If a participant received an injury while playing handball, they completed a separate section two form per injury. Section two required detail on the location, side, type, mechanism, severity, time, treatment received, outcome, reoccurrence and month of injury. The National Handball Council of Ireland distributed the questionnaire to all secretaries in Ireland for distribution to handball clubs. Ethical approval was granted by Dublin City University Ethics committee. An injury was defined as “one sustained during training or competition resulting in restricted performance or time lost from play”3. A warm up was defined as a period of preparatory exercise designed to “(i) improve a muscle’s dynamics so it’s less inclined to injury; and (ii) prepare the athlete for the demands of exercise”4. Injury severity was defined according to days lost from playing handball and was subdivided into a minor injury (≤7 days), moderate injury (8-21 days) and severe injury (>21 days)5.
Results
Participants were primarily male (89.3%) with only 10.7% female handball players partaking. The mean age was found to be 36.7±15.7 years and the mean years of playing handball was 19.1±14.6 years. The mean Body Mass Index (BMI) was 25.2±4.3kg/m² for all participants with females (23.6±5.8kg/m²) presenting with a lower BMI than males (25.4±4.1kg/m²). 35.6% of participants played 40/20 only, 26% played both 40/20 and 60/30, 9.7% played 40/20, 60/30and One-Wall and 2.7% played all four codes of handball. If the total number of participants that play each code of handball is calculated, 68 played the 40/20code, 35 played the 60/30 code, 14 played hardball and 14 played one-wall. The most common level of handball played by the participants was masters(27.9%) followed by junior (26.2%) and intermediate (16.4%).85.1% were right hand dominant, 4.1% were left hand dominant and 10.8% were ambidextrous for handball. Participants spent a mean of 4.1± 2.1 hours playing handball per week. The majority (85.1%) of participants completed a warm-up with the mean duration 10.8±5.9 minutes. 41.9% wore eye goggles, gloves and glove lining, 23% wore both eye goggles and gloves while 9.5% wore eye goggles alone. If the total number of the participants that wore each type of protective equipment is calculated, 67 participants wore eye goggles, 61 participants wore gloves and 36 participants used glove lining.68.5% of participants also played other sports.
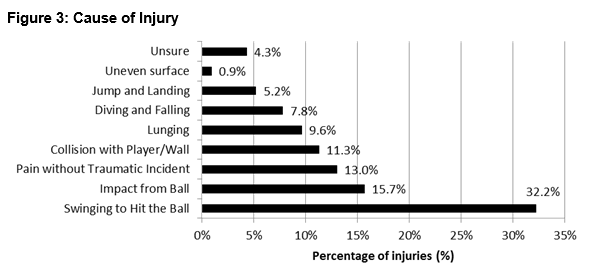
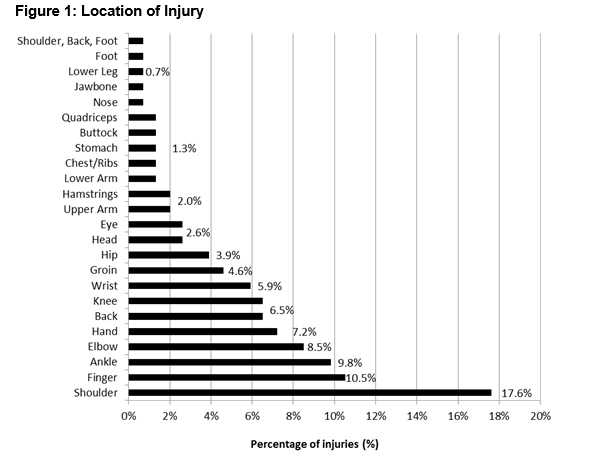
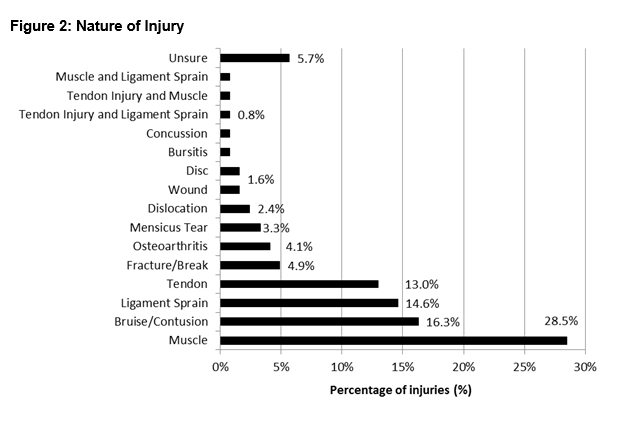
The majority of participants (88%) sustained an injury during their handball career, with a total of 155 reported injuries. Injuries primarily occurred in the upper limb (52.9%), 30.3% in the lower limb and 16.8%in the trunk and head. The most common location for an injury was the shoulder, followed by the finger and ankle (Figure 1). The majority of injuries occurred on the right side (67.3%), 23% on the left and 9.7% bilateral. December (9.7%), January (9.7%), February (9.7%) and November (8.7%) were the most common months to become injured. Injury predominantly occurred during a game (82.4%), followed by a training session (13.6%), warm-up (1.4%) and cooldown (0.7%). Muscle strains were predominant followed by bruise/contusions, ligament sprains and tendon injuries (Figure 2). Swinging to hit the ball was the primary cause of injury, followed by impact from the ball, pain without a traumatic incidence and collision with player/wall (Figure 3). Participants predominantly temporarily discontinued playing/training (61.7%) because of the injury. Injuries were primarily severe (54.7%), followed by moderate (31.3%) and minor (14.1%).67.4% of injuries required treatment by a medical professional and 14.6% of participants were admitted to hospital due to the injury. 19.2% reported the injury as a reoccurring old injury, with 68% of reoccurring injuries originally due to playing handball and 32% due to injury that occurred in another sport or activity of daily living.
Discussion
Handball has been thought to be a male orientated sport1 which is supported by this study. While handball players most commonly play the40/20 code of handball, a large amount of participants also play a combination of codes. Each code has a different season and their competitions takes place at different times during the year. Thus handball players could be required to play in effect two, three or even four season’s worth of matches. Participants predominantly played at the masters’ level, but combinations of levels were also commonly played. Thus, some participants are not only playing different codes of handball but also playing at various levels. However, the low hours spent in training each week indicates that handball tends to be largely recreational. Participants reported a similar right hand dominance to male (82%) and female (91%) veteran tennis players6. The right hand dominance noted may be related to the high incidence of injury on the right side and further research between side of injury and dominance in handball is recommended. Ambidextrous players were more common than left hand dominant players, which is expected as this is advantageous to performance in handball. While the majority of participants completed some form of a warm-up, it was slightly lower than athletes playing upper body sports (91.7%)7 or adolescent squash players (93%)8. Handball players tend to warm up for a duration close to the recommended 10-15 minutes, but at the lower scale of the recommendation9.
Eye goggles, gloves and glove lining were the most commonly used protective equipment worn together while playing handball. The wide use of eye goggles is expected, as they are mandatory in the 40/20 code of handball. While gloves are mandatory in the 40/20 code of handball, they are primarily used to keep the ball dry rather than for injury prevention purposes. Since bruises/contusions were common, the introduction of glove lining, especially in hardball where the ball is harder than other codes could help reduce injuries to the hand and fingers. Injuries were predominant in the upper limb which is expected due to the demands of the game where the use of the upper limb is an integral component of the game. Injuries primarily occurred in the shoulder and a similar percentage of injuries is reported in tennis (12-17%)10. The ankle was also commonly injured in handball, with a similar percentage occurring in tennis (7%)10. Notably only 2.6% of injuries occurred to the eye, which indicates that the mandatory use of eye goggles is effectively preventing eye injuries in handball. Soft tissue injuries were predominant, with muscle strains, bruise/contusions and ligament sprains common. Muscle strains were also the primary nature of injury received in badminton, however they were more frequent (64%)11 than in handball. A similar percentage of ligament strains (14.4%) occurred inbadminton11, however bruises/contusions were far more common in handball. This high incidence of bruises/contusions could be due to the size, nature and speed of the ball used in handball1.Serious injuries like fractures/breaks were not as common as soft tissue injuries and only accounted for 4.9% of injuries.
Swinging to hit the ball was the most common cause of injury which could be related to the large number of upper limb and shoulder injuries. Swinging to hit a ball has been identified as a possible risk factor for injury in overhead sports due to inappropriate swing mechanics coupled with the repetitive nature of the swinging action12. Impact from the ball was also frequent and may be related to the large amount of bruises/contusions noted, thus the introduction of protective pads could reduce injuries. Pain without traumatic incident was common and may be related to overuse injuries due to inappropriate training or defective biomechanics. Collisions with a player/wall were common in handball and may be related to tactics, as players aim to skim the ball along the side wall to make it more difficult for their opponents to return the ball. The four most common months injury occurs corresponds to the beginning (November/December) and height (January/February) of the 40/20 season where players would play an increased number and enhanced intensity of games. Injuries primarily occurred during games, which is expected as intensity is increased and there are usually much larger physical and physiological stresses placed on the athlete which could increase injury risk11. Surprisingly, a large percentage of handball players continued to play/train regardless of receiving an injury despite the risk of further exacerbating the original injury. Out of the61.7% participants who discontinued playing/training, severe injuries predominated, however, it has been demonstrated that participants tend to only remember and report more serious injuries that require prolonged absence from sport in retrospective studies13,14. Thus further prospective research is required. A fifth of injuries were a reoccurrence of a previous injury, which may be due to incomplete rehabilitation, unidentified biomechanical deficiencies or training errors15.
There are a number of limitations to the current study. This is a retrospective study which is considered inferior to a prospective research design as they are less reliable due to recall bias and imprecise estimations of the injury13,16. However, as this is the first study of its kind on the epidemiology of injuries in handball, the information provided is still beneficial. The injury data was gathered using a self-report questionnaire which may not be entirely accurate and may overestimate the severity of the injury17. In addition, injury rate was calculated as a percentage only due to the method of data collection used, and so exposure to handball could not be taken into account. While the percentage of injury reported is related to injuries suffered directly due to handball, 68.5% of those who completed the questionnaire were involved in other sports which may have exacerbated or contributed to the injuries. Despite the limitations of this retrospective study, it has demonstrated that injuries are common in handball with 88% of all participants sustaining an injury. The epidemiological data presented in the current study is the first of its kind in Gaelic handball and so the current authors propose that prospective epidemiological studies should be implemented. Further research on risk factors for injury and injury prevention strategies specific to handball should be designed.
Correspondence:
S O Connor
Department of Life and Physical Sciences, Athlone Institute of Technology, Dublin Road, Athlone, Co Westmeath
Email: [email protected]
Acknowledgements:
Comhairle Liathróid Láimhe na hÉireann for their assistance in the distribution of the questionnaire.
References
1. hÉireann CLLn. The four handball codes. http://www.handball.ie/four_codes; 2009 [cited 200922/01/2009].
2. van Mechelen W. Sports injury surveillance systems. Sports Medicine. 1997;24:164-8.
3. Cromwell F, Walsh J, Gormley J. A pilot study examining injuries in elite gaelic footballers. British Journal of Sports Medicine. 2000;34:104-8.
4. Woods K, Bishop P, Jones E. Warm-up and stretching in the prevention of muscular injury. Sports Medicine.2007;37:1089-99.
5. Newell M, Grant S, Henry A, Newel J. Incidence of injury in elite gaelic footballers. Irish Medical Journal.2006;99:269-71.
6. Brasseur J-L, Lucidarme O, Tardieu M,Tordeur M, Montalvan B, Parier J, et al. Ultrasonographic rotator-cuff changes in veteran tennis players: the effect of hand dominance and comparison with clinical findings. European Radiology. 2004;14:857-64.
7. Lo YP, Hsu YC, Chan KM. Epidemiology of shoulder impingement in upper arm sports events. British Journal of Sports Medicine. 1990;24:173-7.
8. Meyer L, van Niekerk L, Prinsloo E, Steenkamp M, Louw Q. Prevalence of musculoskeletal injuries among adolescent squash players in the Western Cape. South African Journal of Sports Medicine.2009;19:3-8.
9. Midgley AW, Mc Naughton LR. Time at or near VO2max during continuous and intermittent running: a review with special reference to considerations for the optimisation of training protocols to elicit the longest time at or near VO2max. Journal of Sports Medicine and Physical Fitness. 2006;46:1-14.
10. Abrams GD, Renstrom PA, Safran MR. Epidemiology of musculoskeletal injury in the tennis player. British Journal of Sports Medicine. 2012;46:492-8.
11. Yung PS-H, Chan RH-K, Wong FC-Y, Cheuk PW-L, Fong DT-P. Epidemiology of injuries in Hong Kong elite badminton athletes. Research in Sports Medicine. 2007;15:133-46.
12. Abrams GD, Sheets AL, Andriacchi TP, Safran MR. Review of tennis serve motion analysis and the biomechanics of three serve types with implications for injury. Sports Biomechanics.2011;10:378-90.
13. Junge A, Dvorak J. Influence of definition and data collection on the incidence of injuries in football. The American Journal of Sports Medicine. 2000;28:S-40-S-6.
14. Twellaar M, Verstappen FTJ, Huson A. Is prevention of sports injuries a realistic goal? A four-year prospective investigation of sports injuries among physical education students. The American Journal of Sports Medicine. 1996;24:528-34.
15. Di Fiori JP. Overuse injuries in children and adolescents. Physician and Sports Medicine. 1999;27:75-90.
16. Inklaar H. Soccer injuries. Sports Medicine. 1994;18:55-73.
17. Grossman J, Jamieson J, Hume KM. Perceptions of athletic injuries by athletes, coaches, and medical professionals. Perceptual and Motor Skills. 1990;71:848-50.
p370