Introduction
Road traffic injuries are a major public health problem, requiring concerted efforts for effective and sustainable prevention. 96% of all children killed worldwide as a result of road traffic injuries occur in low- and middle-income countries1-4. The required strategy to reduce the road toll involves the identification of the problem, the formulation of a strategy, setting targets and thereafter the monitoring of performance. Our aim with this study was to assess the rates of road-related fatalities and injuries in a paediatric population over three 5-year time periods. We hoped to assess the differences, if any, in the injury and fatality rates and to assess the likely causes associated with these results.
Methods
All road and traffic collisions requiring police assistance occurring on public roads in Ireland in three separate time periods spanning five years (1996-2000, 2004-2008 and 2009-2013) were included. Accident details are recorded by the attending police officer on the CT [68] form. This form collects information on severity of the accident, road user category, contributing factors such as road factors, vehicle factors, environmental factors and also what safety precautions were in place at the time of the accident (such as seatbelt use, bicycle helmet use and pedestrian data). The information was then entered into an SPSS database and accident trends were analysed and reviewed by the Research Section of the Road Safety Authority. Injuries were sub-classified as fatalities, serious [those admitted to hospital, fractures, severe head injuries, severe internal injuries or shock requiring treatment] and minor. From this database we sought information pertaining to those children and adolescents aged fifteen years and younger. We then compared the results from the initial cohort in 1996-2000 with both 2004-2008 and 2009-2013.
Results
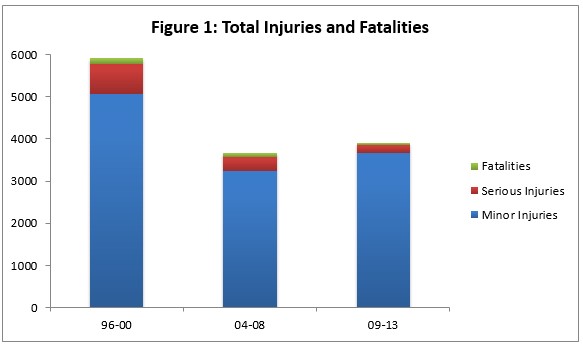
When we compared the three study periods (Table 1) we found that there was a decrease in the total number of children injured or killed on our roads from 5928 to 3903 (Figure 1). Minor injuries fell by from 5,063 to 3,659, serious injuries fell from 712 to 201 and fatal injuries by from 163 to 43 (a 72% drop).
Car passenger fatalities
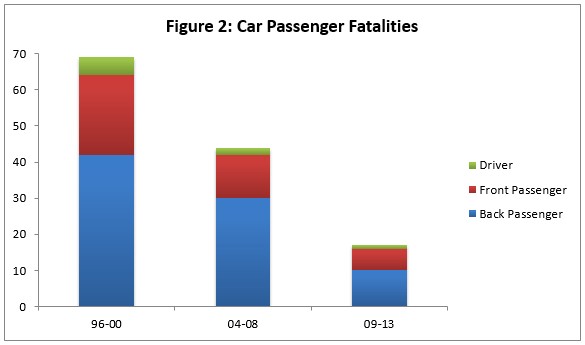
Car passenger fatalities fell from 69 (1996-2000) to 44 (2004-2008) and 17 (2009-2013 (Figure 2). The majority of these children were travelling in the rear seat however 7 of 17 car passenger fatalities were front seat passengers and 25 of 92 serious injuries were front seat passengers.
Pedestrian Injuries
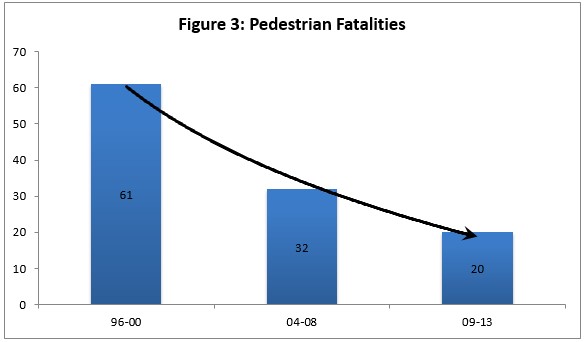
There was a slight rise in pedestrian injuries from the 2004-2008 cohort (1232) to the 2009-2013 cohort (1258) but pedestrian deaths fell from 61 (1996-2000) to 32 (2004-2008) with a further welcome drop to 20 (2009-2013) (Figure 3). Pedestrian injuries which accounted for 32% of the total injury toll.
Cyclist Injuries
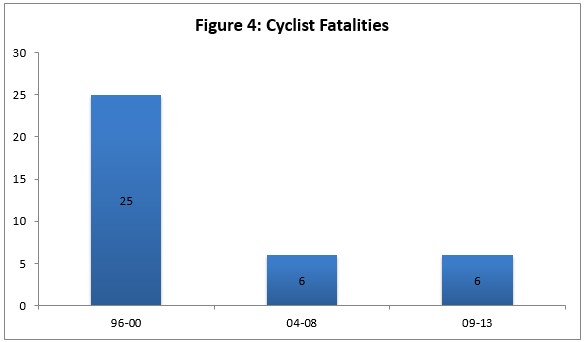
Cyclist fatalities fell from 25 (1996-2000) to 6 (2004-2008) but remained at 6 (2009-2013) reflecting a disappointing halt in progress. (Figure 4) In contrast to previous years none of the fatalities in this category were under the age of 10. There was no information available on the use of helmets in any of the fatalities.
Discussion
In terms of road safety measures, policies including legislation and regulation that prohibit risky behaviours can be effective in shifting social norms1. The likelihood of the adoption of effective national policies regarding road safety is enhanced by an understanding public opinion2,3. Twenty miles per hour speed zones have shown4,5 a very significant reduction in pedestrian fatalities and serious injuries especially in the under-5 age group. Road traffic collisions are a major cause of childhood death throughout the EU1,.
Road deaths are only the tip of the iceberg of the burden of road crashes. Injured road users represent an increasing concern for public authorities, given the burden they impose on national health systems. Long-lasting injuries often leading to disability are a significant problem. The use of a seat belt reduces the probability of fatal injury in a crash by more than 50%. Similarly, the use of helmets by users of two-wheeled vehicles has a huge life-saving potential.
The most positive changes to road user behaviour happen when road safety legislation is supported by strong and sustained enforcement, and where the public is made aware of the reasons behind the new law and the consequences of noncompliance. Enforcement of speed limits is essential to make them truly effective6,7. Children in an appropriate restraint8 are significantly less likely to be killed or injured than unrestrained children, and are also less likely to be killed or injured than children using adult seat-belts. Rear-facing restraints for babies and infants (under one year) have been shown to reduce the risk of death or injury by 90% compared to being unrestrained. Children in booster seats, generally aged four to ten years, have a 77% reduced risk of being injured in a crash compared to unrestrained children .Mobile phone use (including texting)creates various types of distraction: visual, auditory, manual and cognitive9,10.
In terms of this study, we have determined that across all categories there has been a marked reduction in childhood injuries and fatalities on Irish roads in the years 2009-2013 in comparison to1996-2000. Comprehensive and clear legislation, enforced with appropriate penalties and accompanied by public awareness campaigns, has been shown to be a critical factor in reducing road fatalities associated with speed, drink driving and the failure to use appropriate restraints in cars11,12,13,14,15,16.
Widespread random breath testing, as applied to at least one in ten drivers every year in Australia, achieves the highest compliance with laws setting blood alcohol (BAC) levels7. Enforcement should be unpredictable as to time and place (not just holiday periods!) so drivers cannot avoid being tested10,12. We know that speed kills and safe speed thresholds vary according to different types of road, weather and light conditions and that pedestrians have a 90% chance of surviving if knocked down by a car travelling at 30 km/hour and this drops to less than 50% if car speed is 45 km/hour or above13-15,16. Effective interventions to increase child restraint use include laws mandating use of child restraints, public information and enhanced enforcement campaigns, public education programmes to support enforcement and child restraint loan schemes. In order to avoid lap belt syndrome18, booster cushions are required in the 6-11 year old age group.
The use of bicycle helmets has been found to reduce the risk of head and brain injuries by between 63% and 88%16. A meta-analysis of studies has shown that the mandatory wearing of bicycle helmets reduced the number of head injuries among cyclists by 25%17. Evaluation of bicycle helmet legislation has been encouraging and there is now unequivocal evidence that helmets reduce the incidence and severity of head, brain and upper facial injuries in children.
Road traffic injuries in children are predictable and therefore preventable and to reduce the injury toll further requires a coordinated and collaborative effort across many sectors18. The success of the past 17 years should act as a spur to further reduce this toll in our vulnerable road users.
Conflicts of Interest
I have no conflicts of interest in this paper
Correspondence:
Prof A Nicholson, RCSI Department, Temple Street Children’s University Hospital, Dublin 1
Email: [email protected]
References
1. World report on road traffic injury prevention published by WHO and the World Bank for World Health Day 2004.
2. Clegg Smith K, Debinski B, Pollack K, Vernick J, Bowman S Samuels AGielen A. Research – informed evidence and support for road safety legislation: Findings from a national survey. Accident analysis and Prevention 2014 ; 73: 109-115
3. Strategies to prevent unintentional injuries among children and young people aged under 15. NHS Evidence Update 29 February 2013
4. Grundy C, Steinbach R, Edwards P, Green J, Wilkinson P. Effect of 20mph traffic speed zones on road injuries in London 1986-2006 : controlled interrupted time series analysis. BMJ 2009 ; 339: b4469
5. WHO Global Report on Road Safety 2015
6. European Transport Safety Council. Setting appropriate, safe and credible speed limits. Brussels: ETSC; 2010
7. Durbin D, Chen I, Smith R, Elliott MR, Winston FK. The effect of seating position and appropriate restraint use on the risk of injury to children in motor vehicle crashes. Pediatrics 2005; 115; e305-e309
8. Redelmeier DA, Tibshirani RJ, Evans L. Traffic law enforcement and risk of death from motor vehicle crashes: crossover study. Lancet 2003; 361: 2177-2182
9. Dragutinovic N, Twisk D. Use of mobile phones while driving – effects on road safety. Leidschendam, Netherlands: SWOV Institute for Road Safety Research 2005. BMJ 2002; 324: 1145-1148
10. Caird J. A meta-analysis of the effects of texting on driving. Accidental Analysis and Prevention. 2014;71: 311-318.
11. Laflamme L, Diderichsen F. Social differences in traffic injury risk in childhood and youth: a literature review and research agenda. Injury Prevention 2000; 6: 293-298.
12. Williams AF, Ferguson SA. Rationale for graduated licensing and the risks it should address. Injury Prevention 2002; 8: 9-16.
13. Bunn F, Collier T, Frost C, Ker K, Roberts I, Wentz R. Traffic calming for the prevention of road traffic injuries: review and meta-analysis. Injury Prevention 2002; 9: 200-204.
14. Crandall JR, Bhalla KS, Madely J. Designing road vehicles for pedestrian protection. BMJ 200; 324: 1145-1148.
15. Redelmeier DA< Tibshirani RJ, Evans L. Traffic law enforcement and risk of death from motor vehicle crashes: crossover study. Lancet 2003; 361: 2177-2182.
16. Thompson DC, Rivara FP, Thompson R. helmets for preventing head and facial injuries in bicyclists. Cochrane Database of Systematic reviews 2000; CD 001855.
17. Macpherson AK, To TM, Macarthur C, Chipman ML Wright JG, Parkin PC. Impact of mandatory helmet legislation on bicycle-related head injuries in children: population based study. Pediatrics 2000; 110: e60.
18. Elvik R, Vaa T. Handbook of road safety measures. Amsterdam Elsevier 2008.
(P728)