Case Study
An 82-year-old male, with a background of COPD, presented to the emergency department complaining of progressive dyspnea and dysphonia. On initial evaluation it became rapidly apparent that he was in significant respiratory distress, with audible stridor. Flexible nasendoscopy confirmed upper airway obstruction with a large submucosal mass obstructing the laryngeal inlet. An emergency tracheotomy was performed in order to secure the airway.
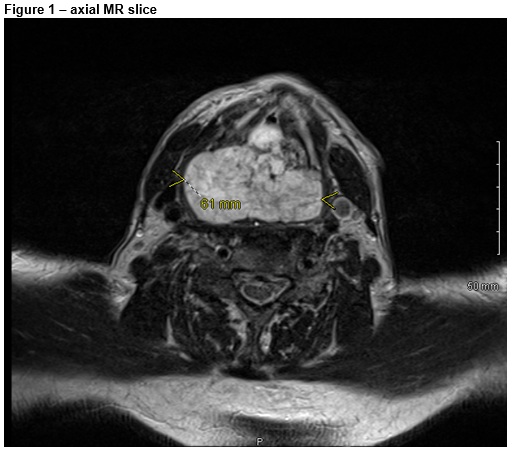
CT scan and core biopsy of the mass were performed, after which he was transferred to a tertiary unit for further investigation and management. Imaging (CT & MR) demonstrated a large mass, measuring 7.5 x 6.6 x 4.0cm, centered on the cricoid cartilage, with extensive cartilaginous destruction, without evidence of cervical lymphadenopathy.
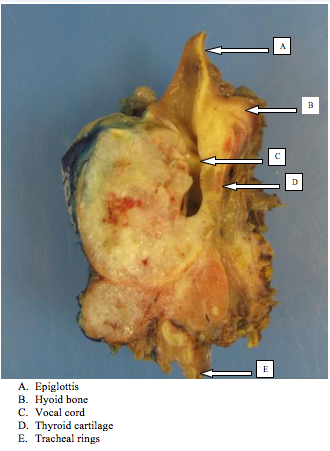
Histological scrutiny of the biopsy demonstrated a hypercellular cartilaginous tumour, with mild to moderate pleomorphism. Closer inspection demonstrated mitotic cells, with a frequency of approximately one per 10 high power fields. Despite these features a formal histologic diagnosis couldn’t be reached, based on limited size of the biopsy specimen. Repeat biopsy demonstrated similar features however a diagnosis remained elusive. The case was discussed at the local head and neck oncology MDT. Based on imaging and histology, total laryngectomy was recommended. (Figure 2 – laryngectomy specimen)
The patient elected to proceed and had an uneventful post-operative course. Following speech rehabilitation with a speaking valve he was discharged. He had follow up at 6 weeks and 6 months, and was doing well. He will continue to be followed up yearly for at least 5 years.Final histology confirmed the diagnosis of a grade 1 chondrosarcoma with evidence of some areas of transition to grade 2.
Discussion
Laryngeal cancer is relatively uncommon, encompassing around 1% of all cancers. Of these, squamous cell carcinoma accounts for the majority, with a high male:female perponderance (5:1)1. Chondrosarcoma accounts for around one percent2. It usually presents with classic signs and symptoms of a laryngeal tumour; ie dysphonia, inspiratory stridor, dysphagia, odynophagia, neck mass, or persistent cough3. It is usually a slow growing tumour and therefore rarely presents with acute airway obstruction. It is most commonly centred on the cricoid cartilage (70 – 75%), however it can also arise from the thyroid cartilage, epiglottis and arytenoids in descending order of incidence4.
Symptoms depend on the location. Subglottic and endolaryngeal tumours will generally cause dyspnoea. Extralaryngeal tumours may compress the oesophagus resulting in dysphagia5. In our case the patient presented with inspiratory stridor and mild dysphonia, due to its location originating outside of the larynx, ultimately resulting in laryngeal obstruction due to its sheer size. Diagnosis of laryngeal chondrosacoma can be difficult due its rarity, and that it can be troublesome to differentiate from a benign chondroma2. To diagnose a well differentiated chondrosarcoma, the presence of binucleated chondrocytes is required. Most studies cite this definition to make the distinction between well-differentiated chondrosarcoma and chondroma6. Once a diagnosis of chondrosarcoma has been made, it is further subcharacterized into grade 1, 2 or 3, based on the criteria below, summed up by Lichtenstein and Jaffe:
Grade 1 – Similar to a chondroma, more than two nuclei, no mitoses, some areas of calcification and actual bone tissue.
Grade 2 – Incease in cell number, low nuclear/cytoplasmic ratio, scarce mitoses.
Grade 3 – Multinucleated cells, increased nuclear/cytoplasmic ratio, high number of mitoses7.
Laryngeal chondrosarcoma has favourable prognosis compared to other laryngeal cancers, largely due metastases being rare. Despite this these tumours can often be locally aggressive, resulting in local invasion and, as it did in our case, causing airway compromise2,3,8. Given that distant metastases are so rare, adjuvant chemotherapy is rarely considered3,7. Radiotherapy is also considered to be of limited benefit in laryngeal chondrosarcoma, as it is poorly radiosensistive. There are however some conflicting reports regarding its adjuvant use in cases with residual disease after surgery9,10.
In conclusion, laryngeal chondrosarcoma is a rare form of laryngeal cancer. Its diagnosis is aided by appropriate imaging and close scrutiny of histological samples, ideally by experienced pathologists with an expertise in head and neck malignancy and/or soft tissue masses. Radical surgery is usually necessary but prognosis is generally favourable compared to other laryngeal cancers.
Conflict of Interest
The authors confirm no conflict of interest
Acknowledgements
M Toner, Histopathology Department, St. James’ Hospital
Correspondence:
Kilian Tuite, St. James’ Hospital, Dublin, Ireland
Email: [email protected]
References
1] www.cancer.net, available at http://www.cancer.net/cancer-types/laryngeal-and-hypopharyngeal-cancer/overview
[2] Dubal PM, Svider PF, Kanumuri VV, Patel AA, Baredes S, Eloy JA. ‘Laryngeal Chondrosarcoma: A Population Based Analysis’. The Laryngoscope, 124:1877-1881, 2014
[3] Williamson JS, Biggs TC, Ingrams D. ‘Laryngeal Cancer, an Overview’. Trends in Urology and Mens Health, November/December 2012.
[4] Moerman M, Kreps B, Forsyth R. ‘Laryngeal Chondrosarcoma: An Exceptional Localisation of a Not Unfrequent Bone Tumor’. Sarcoma, Volume 2009 (2009), Article ID 394908\
[5] Sakai O, Curtin HD, Faquin WC, Fabian RL. ‘Dedifferentiated Chondrosarcoma of the Larynx’. American Journal of Neuroradiology. 21:584-586, March 2000.
[6] Torbaghan SS, Ashouri M, Naderi NJ, Baherini N. ‘Histopathologic Differentiation between Enchondroma and Well-differentiated Chondrosarcoma: Evaluating the Efficacy of Diagnostic Histologic Structures’ Journal of Dental Research, Dental Clinics, Dental Prospects. 2011 Summer; 5(3): 98–101.
[7] Buda I, Hod R, Feinmesser R, Shvero J. ‘Chondrosarcoma of the Larynx’. Israel Medical Association 2012; 14: 681-684
[8] Sauter A, Bersch C, Lambert KL, Hormann K, Naim R. ‘Chondrosarcoma of the Larynx and Review of the Literature’, Anticancer Research, 27: 2925-2930. 2007.
[9] Gelderblom H, Hogendoorn PCW, Dijkstra SD, Van Rijswijk CS, Krol AD, Taminiau AH, Bovée JV. ‘The Clinical Approach Towards Chondrosarcoma’. The Oncologist. March 2008. 13: 320-329
[10] Lee SY, Lim YC, Song MH, Seok JY, Lee WS, Choi EC. “Chondrosarcoma of the Head and Neck’. Yonsei Medical Journal, 2005 April 30; 46(2): 228–232
P676