Case Report
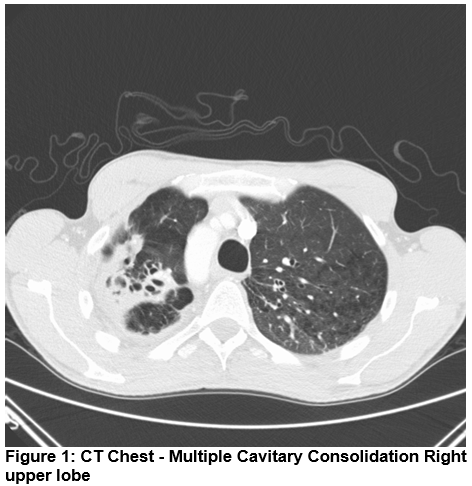
A 38 Year old gentleman, truck driver by occupation, presented with productive cough, shortness of breath on exertion & night sweats of 15 days duration. He had joint pains with rash affecting ankle joints for 15 days which resolved spontaneously. He was a keen football player and would feel short of breath whilst playing football in the three months prior to presentation. He attributed this to smoking. He smoked 3 packs/day for 15 years. There was no history of sexual promiscuity, drug or alcohol abuse. He had tattoos over both arms. His background history was significant for a spontaneous Pneumothorax treated conservatively 18 years ago. There was no history of Pulmonary TB or TB exposure in the past. He was BCG vaccinated. There was no family history of Emphysema or Liver disease. His Chest X Ray showed Right upper zone infiltrates. His CT Thorax shows bilateral extensive emphysematous lung disease with Right upper lobe infiltrates.
Laboratory results: 2 sputum samples were positive for AFB (+++). However Gene Xpert test for Mycobacterium Tuberculosis was negative. Quantiferon assay was negative. Bronchoalveolar lavage & washings sent for AFB smear & culture showed growth of Non tuberculous Mycobacteria identified as M .Malmoense. Drug sensitivity testing was done & decision to treat was taken in expert consultation with the Microbiology Department at Waterford. The decision to treat was guided by the positive CT Findings and recurrent positive AFB growth. Pulmonary Function Test were normal. Alpha-1 antitrypsin levels were normal & genetic testing revealed a normal MM phenotype. Patient has been counselled and encouraged about smoking cessation.
Discussion
Pulmonary infections with NTM occur in patients with or without predisposing conditions and recognition of this disease is delayed due to its indolent nature3. Symptoms & signs are non-specific. Fever & weight loss occur less frequently than in patients with typical tuberculosis. Since these infections frequently coexist with underlying lung disease such as COPD or Bronchiectasis, physical findings of the latter disease may predominate4,5. In our case report, findings of underlying emphysematous lung disease were subtle & symptoms of shortness of breath on exertion was elicited only on further probing. Laboratory results in our patient showing persistent sputum for AFB positive & Gene Xpert for M. Tuberculosis negative raised a diagnostic dilemma both in terms of isolation of the patient & treatment involved7. Final diagnosis of M. Malmoense infection was made as the BAL specimen confirmed growth on culture
As suggested by ATS/IDSA guidelines, Expert consultation should be obtained when NTM are recovered. Patients who are suspected of having NTM lung disease, but do not meet diagnostic criteria should be followed until the diagnosis is finally established or excluded6,8. Making the diagnosis of NTM lung disease does not per se necessitate the institution of therapy, which is a decision based on potential risk & benefits of therapy for symptomatic patients.
Conflict of Interest:
The authors confirm no conflict of interest.
Correspondence: Nitish Marathe, Respiratory Department, St Luke’s General Hospital, Freshford Rd, Kilkenny
Email: [email protected]
Acknowledgements
B Lynch, Microbiology Department, Waterford Regional Hospital
References
1. Griffith DF, Aksamith T, Bown-Elleott BA Catanzaro A,Daley C,Gordin F,Holland SM,Horsburgh R,Huitt G,Iademarco MF,Iseman M,Olivier K,Ruoss S,Von Reyn CF,Wallace RJ Jr,Winthrop K. An official ATS/IDSA statement: diagnosis, treatment & prevention of Nontuberculous Mycobacterial disease .AMJ Respiratory Critical care Med 2007; 175:367.
2. Dardson PT. The diagnosis & management of disease caused by M.Avium Complex, M.Kansasii & other Mycobacterium. Clinical Chest Me 1989;10:431
3. Prince DS,Peterson DD,Steiner RM,Jonathan E,Richard Scott,James E.Fish. Infection with Mycobacterium Avium Complex in patients without predisposing conditions. New England Journal of Medicine 1989; 321:863
4. Ahn CH, Mcharty JW,Ah SS,George A Hurst. Diagnostic criteria for Pulmonary disease caused by Mycobacterium Kansasii & Mycobacterium Intracellulare. Am Rev Respiratory Disease 1982; 125:388
5. Teirsfein AS, Damsker B, Kirschner PA. Pulmonary infection with Mycobacterium Avium Interacellulare; diagnosis, clinical patterns, treatment. Mt Sinai J Med 1990; 57:209.
6. Christensen EE, DietzGW,Ahn CH,Chapman JS,Murray RC,Hurst GA. Radiographic manifestation of pulmonary Mycobacterium Kansasii infections. AJR Am J Roentgenol 1978; 131:985
7. Nucleic acid amplification tests in the diagnosis of TB. MMWR Moob Mortal weekly Report 2009; 58:7
8. Kohlaenin H, Valtonen X, Tukrasnin p,T.Poussa,J.Eskola & A.Jaruvinen. Prognostic value of American Thoracic Society Criteria for non-tuberculous mycobacterial disease; a retrospective analysis of 120 cases with four year of follow up. Scand J Infectious Disease 2013; 45:194
(p516)