Introduction
Ameloblastic carcinoma is a rare malignant odontogenic tumour, mostly affecting the mandible. The following were the only three cases seen in the Irish National Maxillofacial Unit between 2002 and 2014. En bloc resection with 1-2cm margins affords a local recurrence rate of less than 15%1. There is a clear role for radiotherapy whereas the role of chemotherapy is less apparent2.
Case series
Methods involved retrospectively reviewing clinical notes, radiology and histopathology of three cases. Case one was an 80-year-old male with a 15mm ulcerative swelling at the left lower mandibular alveolus. Biopsy showed ameloblastic carcinoma with associated benign ameloblastoma. Orthopantomogram (OPG) X-ray and mandible X-rays confirmed a 25mm lucent defect. The patient had multiple co-morbidities and elected for radiotherapy alone, receiving 35 fractions at 2Gy per fraction. Clinically, the intraoral ulcerated area reduced by 90%. However, mandibular radiolucency remained unchanged on imaging 5 years later

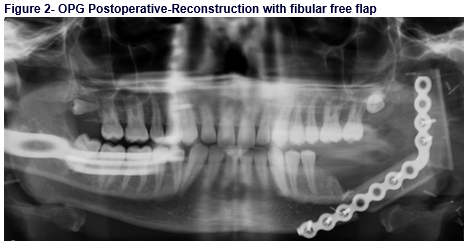
Case two was a 26-year-old male presenting with pain, odynophagia and swelling of the
left ascending ramus. X-rays revealed a lytic lesion in the left mandibular body and ramus. Computed tomography (CT) reported a multiloculated cystic mass (fig 1.). Surgical management involved left partial mandibulectomy and reconstruction with left fibular free flap (fig. 2). Pathological examination of preoperative biopsy and surgical specimen confirmed ameloblastic carcinoma and ameloblastoma. The tumour was 47mm in diameter with clear bony margins. One soft tissue margin was involved. The patient received radiation with a total target dose of 66 Gy with no recurrence at four years.
Case three involved a 64-year-old lady presenting with a 3cm mass on the buccal aspect of the right lower second premolar tooth, associated with paraesthesia and pain in the mental nerve distribution. Imaging showed a three cm radiolucent lesion with no metastases. The patient underwent a hemimandibulectomy, level one and two neck dissections and reconstruction using a left fibular osteocutaneous free flap. Biopsy confirmed an ameloblastic carcinoma. Pathological specimen measured 28mm, with concurrent ameloblastoma. Bone and soft tissue margins were clear with no recurrence at 6 years.
Discussion
Ameloblastic carcinoma is a rare malignant odontogenic neoplasm. It may appear de novo or arise from a pre-existing ameloblastoma or odontogenic cyst. and has a predilection for the mandible over the maxilla3,4. Diagnostic criteria include reverse polarity and palisaded nuclei with malignant cytologic features5. Malignant features include hyperchromatism, atypical nuclei, increased mitotic index, necrosis and neural or vascular invasion. Tumours associated with an ameloblastoma are known as secondary type5.
Management includes conservative, surgical and radiotherapeutic modalities. Controversy still exists regarding best treatment6. Surgical excision is the mainstay in current practice with contention arising regarding adequate surgical margins for clearance. Some literature reviews have advised a 2-3cm bony margin whereas others advise en bloc resection with 1-2cm margins1,7. Philip et al. describes the use of adjuvant radiotherapy in controlling local recurrence with positive margins8. Adjuvant radiotherapy was administered in Case two. Chemotherapy has proven to be ineffective to date9. In conclusion, this is a condition with significant variation regarding presentation and management. The literature surrounding this condition is inadequate to establish gold standards of management at this time. The three cases presented in this case series illustrate a diverse sample of patient demographics and management approaches. We would recommend a minimum of one to 1.5cm bony margins, en bloc resection and composite free flap reconstruction. However, if the margins are positive or close, adjuvant radiotherapy should be considered. In the rare occurrence where a patient is accepting of all treatment modalities besides surgery, the role of primary radiotherapy may play a role. Sufficiently powered studies should be carried out in future to assess the role of primary radiotherapy and its effectiveness in this condition.
Correspondence
Mr. Gerard A. Sheridan, Sch, MB, BCh, BAO, MRCSI, MCh (I), National Maxillofacial unit, St. James’ Hospital, Dublin, Ireland
e-mail: [email protected]
Tel: 0851070944
Conflict of interest
None
Ethical approval:
Confirmed
References
1. Datta R, Winston JS, Diaz-Reyes G, Loree TR, Myers L, Kuriakose MA, Rigual NR, Hicks WL Jr.(2003) Ameloblastic carcinoma: report of an aggressive case with multiple bony metastases. Am J Otolaryngol 24(1):64-69
2. Atkinson CH, Harwood AR, Cummings BJ (1984) Ameloblastoma of the jaw: a reappraisal of the role of megavoltage irradiation. Cancer 53(4):869-873
3. Ram H,Mohammad S 95 ,Husain N,Gupta N (2011)Ameloblastic carcinoma.J Maxillofac Oral Surg. 9(4): 415–419
4. Kruse AL, Zwahlen RA, Gratz KW (2009) New classification of maxillary ameloblastic carcinoma based on an evidence-based literature review over the last 60 years. Head & Neck Oncol, 1:31 doi:10.1186/1758-3284-1-31
5. Barnes L, Eveson J.W, Reichart P, Sidransky D. Pathology and Genetics, Head and Neck tumours, World Health Organisation Classification of Tumours. IARC Press: Lyon 2005 6:287-289
6. Ponnam SR,Srivastava G, Sudhakar G (2012) Ameloblastic Carcinoma with Diverse Histological Features: A Case Report. International Journal of Oral & Maxillofacial Pathology 3(1):60-64
7. Avon SL, McComb J, Clokie C (2003) Ameloblastic carcinoma: case report and literature review. J Can Dent Assoc 69(9):573–576
8. Philip M, Morris C G, WerningJ W, Mendenhall W M. (2005) Radiotherapy in the treatment of ameloblastoma and ameloblastic carcinoma. JHK Coll Radiol. 8:157–161.
9. Bruce RA, Jackson IT (1991) Ameloblastic carcinoma.Report of an aggressive case and review of the literature. J Craniomaxillofac Surg. 19:267–71.
(P639)