Introduction
The VitalPAC™ Early Warning Score (ViEWS)1 has been adopted as the National Early Warning Score in all Irish acute hospitals. To date ViEWS has been validated on adult medical (non-trauma) patients in wards and Emergency Departments (ED), but not in prehospital care2-5. Recently Ebrahimian et al studied Early Warning Scores (EWS) for non-traumatic patients in Emergency Medical Service6. To the best of the authors’ knowledge EWS have not previously been compared with priority assessment tools used in ED triage. In most UK and Irish EDs patients are triaged on arrival using the Manchester Triage System (MTS)7. The MTS relies on vital signs but with the addition of reported pain as a central tenet. A patient presenting with normal vital signs and severe discomfort could by allocated a Category 2. The aim of this observational study is to investigate how prehospital applied ViEWS (Ph-ViEWS) compares with MTS. It is hypothesised that most patients triaged with a MTS of 1 or 2 would have a high ViEWS score of ≥7.
Methods
Ethical approval was granted by the University Hospital Limerick (UHL) Scientific Research Ethics Committee. UHL is a 512 bed, major regional referral hospital for the Mid-West region of Ireland, with 60,000 attendances to the ED annually. The Limerick city National Ambulance Service (NAS) responds to circa 13,000 calls annually, about 50% of which are 999 emergency calls. A retrospective chart review was undertaken on a cohort of high acuity (MTS1&2) non-traumatic adult patients. Patients aged >14 years, transported by NAS were included in this study. Patients in cardio-respiratory arrest, those with mental health or palliative care needs, and with missing data were excluded. For the six month period surveyed, 386 fitted the inclusion criteria, with 272 (69 %) having a complete set of values to enable calculation of the score. The Ph-ViEWS score was retrospectively calculated using scanned anonymous relevant reports copies using Microsoft® Office Excel 2003. SPSS for Windows Version 20 was used to carry out the statistical analysis. The distribution of Ph-ViEWS was tested for normality and described graphically and numerically for all patients by MTS category and by whether or not the patient died within 24 hours. The proportion of patients with a Ph-ViEWS ≥ 7 was compared across categories using a Z test for proportions or Fisher’s exact test. A 5% level of significance was used for all hypothesis tests.
Results
The median age of the patients was 65.5 years (range 14 to 98) and 54% were male.
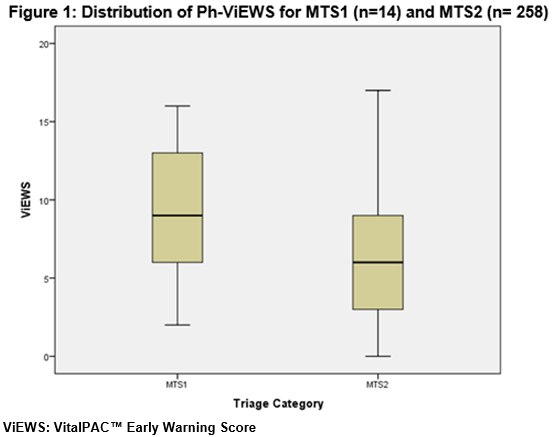
The distribution of Ph-ViEWS was skewed with a median of 6 (range 0 to 17). Of the 272 patients 114 (42%) had scores ≥ 7. The distribution of Ph-ViEWS by MTS category 1 and 2 overlapped and while a higher proportion of MTS1 category patients had scores ≥ 7 compared to those in MTS2, this difference was not significant (64% vs. 41%; p=0.08). Of the 272 patients, 9 (3%) died within 24 hours. The median Ph-ViEWS for these patients was 10 (range 6 to 13) compared to a median of 6 (range 0 to 17) for those who survived. The distribution of Ph-ViEWS by death within 24 hours (yes, no) overlapped but a higher proportion of patients who died had scores ≥ 7 compared to those who were alive at 24 hours (78% vs 41%; p=0.04).
Discussion
In this study, it was found that approximately a third of patients with MTS 1 or 2 in the ED had a Ph-ViEWS below 7. However, it should be noted that all of the patients that died within 24 hours, had presented with a score ≥ 6. Prytherch et al proposed than ViEWS has been validated as a predictor of mortality at 24 hours after stabilisation and admission to a ward, not a predictor of a need for resuscitative care2. The principal limitation of this pilot study is its sample size. Also the study solely focused on high acuity medical patients. A large scale multi-centre study would be required to confirm the findings reported here. In conclusion, ViEWS and MTS are two different systems and are not interchangeable. Practitioners shouldn’t rely on a single Ph-ViEWS measurement to influence their treatment decisions, since it has not been validated for those specific areas of care. More research needs to be undertaken to validate the Ph-ViEWS.
Correspondence: D Gaumont,
National Ambulance Service, Limerick Ambulance Station, Dooradoyle, Co Limerick
Email: [email protected].
Conflict of Interest:
The authors have reported no conflict of interest.
Acknowledgements
J Crowe (NAS paramedic), B Realy (UHL), N Quinn (Nurse Manager UHL), S Walkins (research nurse UHL ED), J Kellett (Physician), the Nursing Staff of UHL ED and C O’Donnell (NAS Medical Director) for their support and contribution to this project.
References
1. Guiding Framework and Policy for the National Early Warning Score System to Recognise and Respond to Clinical Deterioration, 2012. Health Service Executive. Dublin [online] available at: http://www.hse.ie/eng/about/Who/ONMSD/practicedevelopment/MEWS/ewsframework.pdf [downloaded on December 12th, 2012].
2. Prytherch, D. R., Smith, G. B., Schmidt, P. E. and Featherstone, P. I. (2010) 'ViEWS—towards a national early warning score for detecting adult inpatient deterioration', Resuscitation, 81, 932-937.
3. Kellett, J., Woodworth, S., Wang, F. and Huang, W. (2013) 'Changes and their prognostic implications in the abbreviated Vitalpac™ early warning score (ViEWS) after admission to hospital of 18,853 acutely ill medical patients', Resuscitation, 84, 13-20.
4. Groarke, J. D., Gallagher, J., Stack, J., Aftab, A., Dwyer, C., McGovern, R. and Courtney, G. (2008) 'Use of an admission early warning score to predict patient morbidity and mortality and treatment success', Emergency Medicine Journal, 25, 803-806.
p423